

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Analysis of thrombopoiesis is important in evaluating hematologic and non-hematologic diseases. Recent improvements in automated blood cell analyzers allow measurement of several platelet parameters, providing additional information on the underlying mechanisms of thrombocytosis and thrombocytopenia. The ADVIA 2120 Hematology System (Siemens AG, Eschborn, Germany) distinguishes platelets by a two-angle laser light scattering flow-cytometric method [1]. Using the refractive index and a volume histogram, this instrument measures the following platelet parameters: platelet distribution width (PDW), platelet crit (PCT), mean platelet component (MPC), mean platelet mass (MPM), and large platelet count (LPLT), in addition to the total platelet count (PLT) and mean platelet volume (MPV). However, except for PLT and MPV, these parameters are not routinely reported or widely used in clinical practice. Since the importance of these parameters has been increasingly reported, establishing their reference intervals would be valuable [2-5]. However, reference intervals for these platelet parameters are not established in Korea. Therefore, we determined reference intervals for platelet parameters in Korean adults according to the Clinical and Laboratory Standard Institute (CLSI) guidelines [6].
We enrolled 480 adults aged 19-82 yr who visited Gachon University Gil Medical Center for an annual medical checkup from March to July 2012. They consisted of 120 men aged 20-49 yr, 120 women aged 20-49 yr, 120 men aged ≥50 yr, and 120 women aged ≥50 yr. The median age of the study population was 49.5 yr (range, 19-82 yr). In all the subjects, blood test results for complete blood count, chemistry, and blood coagulation were within the reference ranges. For complete blood count, reference ranges were as follows: hemoglobin, 12-16.5 g/dL for women and 13-18.5 g/dL for men; white blood cell counts, 4-10×109/L; and PLT counts, 150-450×109/L. This study was exempt from requiring approval by the institutional ethics committee.
The PLT, MPV, PDW, PCT, MPC, MPM, and LPLT were measured using the ADVIA 2120 Hematology System according to the manufacturer's instructions. Blood samples were collected in EDTA tubes and processed within 4 hr of collection. The ADVIA 2120 calculates MPV from the platelet volume histogram (range, 0-60 fL). The PDW is the distribution width of the platelet volume histogram, while the PCT is the percentage of blood volume engaged by platelets. The MPC is calculated from the platelet component histogram reflective of platelet density (range, 0-40 g/dL), the MPM is calculated from the platelet dry mass histogram (range, 0-5 pg), and the LPLT is the count of platelets larger than 20 fL [1, 7]. The percentage of large platelets (LPLT%) was calculated as (LPLT/PLT) ×100. As recommended by the CLSI guidelines, extreme values lying outside the set of measured reference values were excluded, if the ratio D/R (D=absolute difference between an extreme observation and the next largest observation, R=range of all observation) was equal to or greater than 1/3 [8].
We also assessed whether subdividing the subjects according to age and sex was applicable by the standard normal deviation test as suggested by Harris and Boyd: if z is greater than z*, they recommend partitioning (z=(x1-x2)/[(s12/n1)+(s22/n2)]1/2, where x1 and x2 are the observed means of the 2 subgroups, s1 and s2 are the observed variances, and n1 and n2 are the number of reference values in each subclass, and z* is 3[naverage/120]1/2) [9]. Statistical calculations were performed using SPSS (version 17.0, SPSS Inc., Chicago, IL, USA).
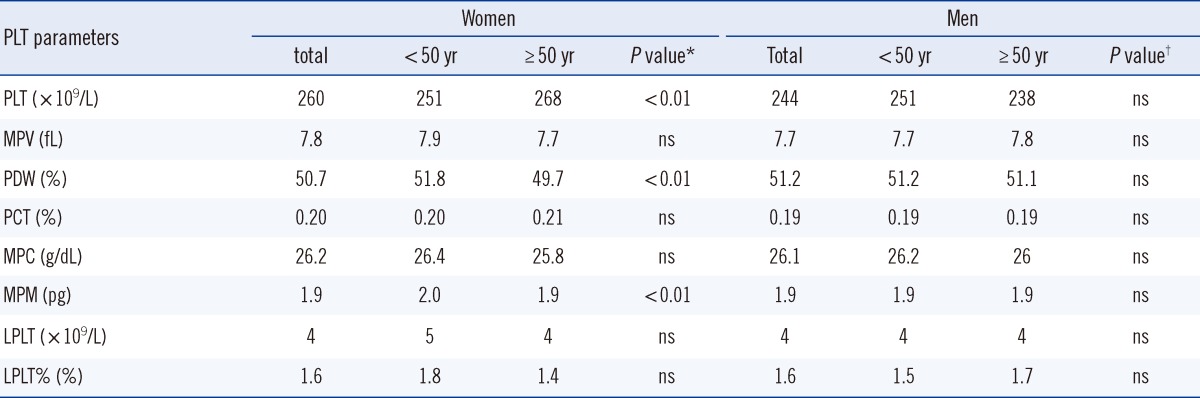
The standard normal deviation test showed that PCT could be divided according to sex. A total of 3 outliers, 1 extreme value each from MPV, PCT, and MPM were excluded from further analyses. All parameters showed non-parametric distributions, and the 2.5th and 97.5th percentiles were taken as reference limits. The reference intervals for each parameter were as follows: MPV, 6.7-9.6 fL; PDW, 39.3-64.7%; PCT, 0.15-0.31% for women and 0.14-0.28% for men; MPC, 22.8-28.0 g/dL; MPM, 1.67-2.29 pg; LPLT, 1-11×109/L; and LPLT%, 0.6-2.9% (Table 1). The median values of each group subdivided by sex and age and P value comparing the median values of different age groups within the same sex using Mann-Whitney test are shown in Table 2.
The median values of PLT were 260×109/L for women and 244×109/L for men. Women had a higher median PLT than men (P<0.01, Mann-Whitney test, data not shown). This finding is in accordance with the results from previous studies using the ADVIA 120, which uses the same method as ADVIA 2120 [1, 10, 11] and another automated analyzer in the United States [12]. The median PCT was also higher for women than for men (P<0.01, Mann-Whitney test, data not shown), which is in agreement with higher PLT in women compared to men in this study and in previous studies [1, 10, 11]. The difference in hormonal profiles may explain the higher PLT counts in women than in men [13]. When the population was subdivided by sex, women older than 50 yr had a higher median PLT than women younger than 50 yr, while the PDW and MPM were lower in older women than in younger women (Table 2).
A few researchers found that men had slightly higher MPV than women [11, 14], while other studies found no statistical difference in MPV between men and women [10, 15]. Similarly, in our study, no difference was found in MPV between men and women. MPV is known as an indicator of platelet activation. As PDW is the distribution width of the platelet volume histogram, it changes along with MPV due to the production of large platelets. MPV and PDW values have been reported to increase in chronic diseases, such as coronary heart disease, diabetes, atherosclerosis, and hypertension [2, 4, 5]. It has been reported that a decrease in MPC indicates stimulation of anticoagulant and thrombin and occurs in the acute stage of ischemic stroke [3].
LPLT and LPLT% apprise the number and percentage, respectively, of immature platelets in the blood stream. To the best of our knowledge, this is the first study to calculate LPLT%. LPLT and LPLT% may be useful to assess thrombopoietic status in thrombocytosis and thrombocytopenia.
This study has several limitations. First, smokers were included in the reference population. However, a previous study indicated that there were no differences in parameters between non-smokers and smokers [10]. Second, subjects with underlying chronic disease such as diabetes and hypertension were also included in the reference population, and their inclusion may affect parameters such as MPV. However, only subjects with normal complete blood count, chemistry, and coagulation tests were included in the reference population; therefore, the impact should be minimal.
Another factor that could affect the parameters is the time interval from sampling to running the analysis. MPV and MPC values are reported to increase when a sample is kept at room temperature for more than 3.5 hr [10]. In our study, the time interval between collection and analysis was approximately 2 to 4 hr; which could have influenced the MPV and MPC. However, the time interval in routine laboratories is likely similar to the intervals reported here.
Last, the reference intervals calculated from data from an analyzer could differ from those used in clinical practice. Thus, these intervals should be considered supplemental data to those used in the clinic.
In conclusion, the reference interval of platelet parameters and median values classified by sex and age in the Korean adults may provide fundamental information about diseases associated with platelets and suggest further avenues for research on platelet parameters.

 XML Download
XML Download