

 PDF
PDF ePub
ePub Citation
Citation Print
Print


It is widely believed that an initial overcorrection is required for the surgical management of intermittent exotropia due to a tendency toward postoperative exodrift [1]. The desired surgical goal in the first week after surgery is to create a small angle of 5 to 10 prism diopters (PD) of esotropia in children with intermittent exotropia [2]. Many ophthalmologists have suggested that initial overcorrection after exotropia surgery in children is necessary for satisfactory long-term correction [34567]. In children, postoperative diplopia is used to stimulate the development of fusional vergences and to stabilize postoperative alignment [2]. However, adults cannot overcome intermittent diplopia induced by overcorrection after surgery for intermittent exotropia. In adults with intermittent exotropia, the first week after surgery usually demonstrates slight undercorrection or orthotropia. The long-term surgical outcome of undercorrection vs. overcorrection in adults remains controversial [89]. The purpose of this study was to evaluate the relationship between initial postoperative overcorrection and long-term surgical success.
Materials and Methods
The study was approved by Gachon University, Gil Medical Center. The medical records of 46 patients who underwent surgery for intermittent exotropia after 18 years of age at Gachon University Gil Medical Center between January 2007 and October 2014 were enrolled and reviewed. The patients also had a postoperative follow-up period of at least 2 years. The records were analyzed for the following data: sex ratio, age at the time of surgery, cycloplegic refractive errors, preoperative angle of deviation, number of patients with good stereoacuity (≤100 arcsec), preoperative stereoacuity, best-corrected visual acuity, duration of postoperative follow-up, and type of surgery. The records were also analyzed to determine the preoperative deviation with stereoacuity and postoperative deviations with stereoacuity during the follow-up examinations at the following intervals: 1 week; 1, 3, and 6 months; and 1 and 2 years [10].
All study examinations were performed by one ophthalmologist (HJP). Visual acuity was assessed after cycloplegic refraction. Ocular alignment was assessed by the use of cover/uncover and alternate prism cover testing at a distance of 20 feet in primary position. Motor alignment at near distance was assessed at 14 inches. To evaluate the sensory outcomes of surgery for intermittent exotropia, stereoacuity was tested with the Titmus stereoacuity test (Stereo Optical, Chicago, IL, USA) and transformed to log arcsec for the purpose of statistical analysis, since stereoacuity thresholds are not on a linear scale. An arbitrary value of 4,500 arcsec (3.65 log arcsec) was assigned to the non-measurable stereopsis. One hundred arcsec was regarded as a reference point for good stereopsis. The questionnaire regarding diplopia asked whether an object appears as two at both near and far distances in primary gaze without abnormal head posture. In addition, patients were asked about binocular diplopia to exclude unilateral diplopia due to postoperative astigmatism.
Intermittent exotropia was defined as divergent strabismus that alternates between phoric and tropic phases. Out of the 4 types of exotropia- basic, convergence insufficiency, pseudo-divergence excess, and true divergence excess-all patients demonstrated only the basic type. Patients with A or V pattern, oblique muscle overactions, or dissociated vertical deviation were not included. The exclusion criteria were a mechanical or neurological cause of strabismus, constant exotropia, previous extraocular muscle surgery, or other ophthalmic or systemic diseases. In addition, patients with exodeviation more than 10 PD at postoperative week 1 were excluded.
The surgical procedure was performed by a single surgeon (HJP) who used the same surgical Park's formula dosage based on the angle of distant deviation for each patient. All patients were examined 1 week after surgery. Postoperative measurements of distance and near deviations were performed at all follow-up examinations in the same manner. On the basis of the initial postoperative deviation at distances measured by prism and alternating-cover test at 1 week, patients were assigned to one of the following groups: group A included patients who showed any esodeviation (−); group B included patients who showed from orthophoria to exodeviation (+) of 10 PD.
Surgical success was defined as an ocular alignment from orthophoria to 10 PD of exodeviation. The rate of exodeviation recurrence, defined as >10 PD of exotropia at distance, was determined by reviewing patient records for up to 2 years after surgery. Analysis of variance was performed by comparing groups A and B based on patient demographic data and preoperative and postoperative angles of deviation. In order to investigate the influence of overcorrection at 1 week postoperatively on long-term surgical success, a preliminary univariate analysis (Fisher exact test or Mann Whitney U-test) was conducted. Statistical analyses were performed using PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA). A p-value less than 0.05 was considered statistically significant.
Results
Forty-six patients with intermittent exotropia were included in this study, 18 (39%) of whom demonstrated some degree of esodeviation (group A), and 28 (73%) showed orthophoria to exodeviation of 10 PD (group B) in the first postoperative week. Of the 46 individuals, 32 were female and 14 were male. The age at the time of surgery ranged from 18 to 64 years, while the average age was 29.6 ± 11.6 years. The mean follow-up period was 28.8 ± 6.1 months. The mean preoperative angle of deviation was 33.4 ± 11.0 PD and ranged from 15 to 50 PD. Fourteen patients underwent recession and resection surgery, 8 patients required unilateral lateral rectus recession; and 24 patients required bilateral lateral rectus recessions (Table 1).
Between the 2 groups, there were no statistically significant differences in sex ratio, age at the time of the surgery, spherical equivalent, preoperative angle of deviation, number of patients with good stereoacuity (≤100 arcsec), preoperative stereoacuity, best-corrected visual acuity, duration of postoperative follow-up, or type of surgery (Table 1).
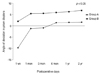
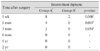
The postoperative angle of deviation for distance fixation up to 2 years after surgery showed a statistically significant difference between the two groups (p < 0.003 in all comparisons). The amount of exodrift for up to 2 years after the operation in group A (from −9.7 ± 6.1 to 1.6 ± 3.7) was greater than that observed in group B (from 2.0 ± 2.7 to 6.8 ± 5.6). In group A, the success rate at each postoperative time increased over the 2 years. In group B, the success rate at each postoperative time decreased and the proportions of recurrence increased during the follow-up period. The long-term surgical success rate within 2 years after surgery was 69% in all patients, 89% in group A, and 57% in group B (p = 0.027) (Table 2 and Fig. 1).
Upon questioning, some patients complained of intermittent diplopia. The number of patients with intermittent diplopia and the duration of diplopia were greater in group A than in group B (Table 3).
Among 46 patients who had completed the final stereopsis test, 26 (57%) demonstrated good stereopsis of 100 arcsec. In group B, two patients showed improved to good stereoacuity of 100 arcsec after surgery. No patients in group A showed improved to good stereoacuity after surgery. Mean stereoacuity throughout 2 years of follow-up did not show statistically significant differences between the groups. However, the improvement of stereoacuity was better in group B (from 2.66 ± 0.75 to 2.40 ± 0.64 log arcsec) than in group A (from 2.56 ± 0.75 to 2.51 ± 0.72 log arcsec) (p = 0.737) (Table 4).
Discussion
Although strabismus surgery is still more commonly performed on children, there has been a significant increase in the number of strabismus operations performed on adults [11]. Studies involving adult exotropia, which should be considered from a different point of view than exotropia in childhood, number many fewer than those of childhood exotropia [9].
The medical records of 46 patients with intermittent exotropia were reviewed. To be included in the study, the patients must have fit the following criteria: undergone surgical correction and followed up for at least 2 years postoperatively. The long-term surgical outcomes from this study indicated that 69% of patients achieved good ocular alignment within 10 PD of exodeviation or orthophoria, and the mean stereoacuity after surgery in the two groups was increased.
Numerous studies have reported that initial postoperative deviation was the only factor found to determine the motor outcome of exotropia in children [512]. Jung et al. [13] showed that overcorrection in adults with exotropia offers a good outcome without side effects. In the present study, the initial postoperative deviation at 1 week after surgery was useful in predicting the overall results of intermittent exotropia surgery for adults. In the overcorrected group 1 week after surgery, 89% of the patients achieved long-term surgical alignment success. For long-term follow-up, the surgical success rate for intermittent exotropia could decrease due to the progression of exodrift, which lasted for 3 to 4 years after surgery [14]. Therefore, overcorrection seems to guarantee a good long-term motor outcome.
There are two aims of strabismus surgery. One aim is to obtain complete balance between the alignment of the two eyes, and the other is to gain binocular vision, including good stereoacuity. Recovery of stereoacuity, which is one factor of binocular vision, improves fine eye movement, maintains the stability of orthophoria, and prevents recurrence [1516]. Orthophoria affects fusion at the stage of binocular vision development. However, Morris and colleagues showed that adults who had not had orthophoria also achieved peripheral fusion after strabismus surgery [17]. Moreover, many investigators have also reported that good stereoacuity could be obtained by other types of strabismus surgery in adults [18192021]. It seems that success in motor alignment leads to better stereoacuity; however, in our study, good stereoacuity was achieved in group B (from 2.66 ± 0.75 to 2.40 ± 0.64 log arcsec), which showed a larger PD than group A (from 2.56 ± 0.75 to 2.51 ± 0.72 log arcsec), with a PD close to zero. According to our results, stereoacuity is not proportional to eye alignment. Diplopia and stereopsis were observed in the overcorrection group for 3 months after surgery, but all individuals showed resolution at 6 months. Stereopsis deterioration due to overcorrection was transient and recovered after several months. Patients who underwent initial overcorrection had the disadvantage of complaining of diplopia for several months; however, after two years, the angle of deviation was closer to orthophoria. In patients with diplopia, occlusion therapy was performed for 1 month after surgery, and prism glasses were prescribed when diplopia persisted thereafter.
This study is limited by the small number of patients and its retrospective nature. Furthermore, there could be a selection bias since we enrolled only patients who were followed for more than 2 years. However, the results of this study could still be valuable, because of the smaller number of patients in group A than group B. Patients with favorable postoperative ocular alignment deviation might not return to the clinic, and this might influence the duration of follow-up. Imaging of the central nervous system was not routinely employed and, in the absence of any abnormality, was not assured. However, any patient whose history or ophthalmologic examination suggested an unrecognized underlying disorder underwent consultation by a neurologist. Furthermore, none of the participants in this study were known to have had a neurologic deficit during the follow-up period.
In conclusion, long-term surgical success was achieved in 89% of patients who were initially overcorrected. Overcorrection of an average of 10 PD at the first postoperative week was found to be associated with a more favorable long-term surgical outcome than undercorrection.



 XML Download
XML Download