

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Bullous keratopathy accounts for the majority of all corneal transplants. Although penetrating keratoplasty (PK) has been the gold standard procedure for bullous keratopathy in the past, Descemet's stripping automated endothelial keratoplasty (DSAEK) has entered the limelight of corneal transplantation because it only replaces the endothelium where the lesion is presented. In addition, studies have shown that DSAEK results in less astigmatism and minimal refractive errors as well as providing for faster visual recovery [1234], elimination of suture related problems, and decreased frequency of wound healing related complications due to the fact that the procedure can be performed through a self-sealing limbal or sclera tunnel incision [5]. Theoretically, DSAEK is also associated with decreased risk of immune rejection of transplanted corneal tissue compared with endothelial keratoplasty because a smaller amount of tissue is transplanted and also because the endothelium is located in what is normally an immune privileged location [6]. While a few long-term clinical studies have been conducted in South Korea, this study is the first attempt to compare long-term clinical outcomes between DSAEK and PK in patients with single preoperative diagnosis of bullous keratopathy.
Materials and Methods
Patients and study design
The present study adhered to the tenets of the Declaration of Helsinki and was approved by the institutional review board of the Catholic University of Korea (KC 15RISI0845). A retrospective medical chart review of patients who underwent DSAEK and PK due to bullous keratopathy at Seoul Saint Mary' Hospital was performed to obtain follow-up data for 2 years between March 2009 and September 2012. Outcome measures included best-corrected visual acuity (BCVA), mean spherical equivalent, spherical and keratometric changes, central corneal thickness as measured with a Tomey pachymeter SP-3000 (Tomey, Nagoya, Japan), endothelial cell density (ECD) measured using a noncontact specular microscope (Konan ROBO-CA, Konan Medical, Hyogo, Japan), and postoperative complications. Intraocular pressure (IOP) was measured using a handheld applanation tonometer Tono-Pen AVIA (Reichert, Depew, NY, USA). Preoperative anterior chamber (AC) depth was measured in each eye with a Tomey ultrasonic biometry UD-6000. PK was performed between the years 2009 and 2011 and DSAEK was performed between 2011 and 2012. Patients with a history of ocular trauma, presence of corneal stromal opacities, uncontrolled glaucoma, or uncontrolled uveitis or other ocular diseases that may have influenced visual outcomes were excluded from our study.
Surgical technique
All DSAEK and PK procedures were performed by CKJ using either general or local retrobulbar anesthesia. All donor tissues were stored in corneal storage solution (Optisol; Bausch & Lomb surgical, Irvine, CA, USA). For preparation of DSAEK lenticules, precut tissue or surgeon-cut tissue was used. In the surgeon-cut method, donor corneas were obtained from the Eye bank of Korea at Seoul Saint Mary's hospital. Precut tissue was imported from Midwest Eye bank, having been prepared by a professional engineer with a microkeratome. In both cases, an 8-mm marker was used for epithelial marking in a circular pattern. Superior corneal incisions of 1 mm were made and after air injection, Descemet's membrane was dissected using a Modified Price-Sinskey hook. A 4-mm temporal scleral tunnel was then made and Descemet's membrane and endothelium were removed from the planned graft area using an I & A system. Next, the donor cornea was dissected with a microkeratome equipped with a 300-µm head and associated artificial AC and was cut to a diameter of 8.25 to 8.75 mm, depending on the recipient corneal diameter. After dissection and punch with a corneal trephine, an anchoring 10-0 Prolene stitch on a long curved needle was placed on the donor disc at the 6 o'clock position. The donor cornea was then placed using the Tan-endoglide method and inserted into the AC. The AC was filled with air for 10 minutes and then part of the air was removed and replaced with balanced salt solution.
The PK procedure was using either general or local retrobulbar anesthesia. An 8-line marker was applied at cornea surface and the donor cornea was trephined using a sharp disposable blade in a guillotine punch block apparatus. The host cornea was trephined to partial thickness using a vacuum trephine and the AC was filled with viscoelastics. The donor corneal tissue was then placed in the host bed properly and four cardinal sutures were placed at the 12, 3, 6, and 9 o'clock positions. Next, 16-bite interrupted sutures were placed with 10-0 nylon. Selective suture removal along the steepest meridian was performed if the astigmatism was greater than 4 diopters (D) in that meridian, beginning 2 months after the surgery.
Postoperative care regimens were the same in both surgical groups, consisting of 0.1% prednisolone (Pred Forte; Allergan, Irvine, CA, USA) and 0.3% gatifloxacin antibiotic (Gatiflo; Handok, Seoul, Korea) eye drops administered four times daily for 2 months. Antibiotic eye drops were discontinued and 0.1% prednisolone eye drops were tapered from twice daily to once daily over a 3-month period.
Data collection and analysis
Study outcome measures consisted of BCVA, spherical and keratometric changes, central corneal thickness, ECD, IOP up to 24 months, and postoperative complications. The data are presented as the mean ± standard deviation and were compared using two-tailed Student's t-tests. The Wilcoxon signed rank test was used to assess the differences between follow-up periods in each group. Mann-Whitney U-tests were used to compare parameters between two procedures. Graft success was assessed by Kaplan-Meier survival analysis. A p-value of less than 0.05 was selected for the threshold of statistical significance. Statistical analyses were performed with IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA).
Results
Among a total of 26 patients (19 males and 7 females) with bullous keratopathy, 15 eyes of 15 patients underwent DSAEK and 11 eyes of 11 patients underwent PK. The mean age was 60.48 ± 10 and 60.17 ± 13 years in DSAEK and PK, respectively. Twelve eyes that underwent DSAEK and 11 eyes of PK were pseudophakic with posterior chamber intraocular lenses. Three eyes that underwent DSAEK were phakic without cataracts at the time of keratoplasty and cataract surgery was not performed during the 2-year follow-up period. Due to the nature of bullous keratopathy, refractive values such as sphere, cylinder, spherical equivalent and ECD were unmeasurable preoperatively in most subjects. There were no comparable differences in preoperative demographics between groups (Table 1). In addition, because of the characteristics of bullous keratopathy, most patients had a greater or lesser degree of corneal opacity before surgery and minor corneal opacity that persisted for the entire follow-up period. Baseline donor characteristics for the two groups are summarized in Table 2. There were no significant differences in mean donor age, death to preservation time, death to operation time, and donor endothelial cell counts between the DSAEK and PK groups.
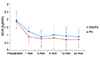
The BCVA before keratoplasty and postoperative 1, 3, 6, 12, and 24 months is presented in Fig. 1. The mean preoperative BCVA was similar in DSAEK and PK (1.89 ± 0.48 vs. 1.95 ± 0.63 logarithm of the minimum angle of resolution [logMAR], respectively, p = 0.241). Both groups showed improvement in visual outcomes after surgery, with better BCVA in the DSAEK group compared with the PK group at all follow-up periods, although the difference was not statistically significant (0.69 ± 0.51 vs. 0.88 ± 0.48 logMAR, respectively at 24 months, p = 0.231).
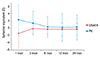
Postoperative refractive and keratometric cylinder measures (D) are shown in Table 3. At postoperative 2 years, the refractive cylinder in DSAEK and PK was −2.60 ± 1.53 and −6.00 ± 1.05 D (p = 0.002), respectively, and the keratometric cylinder was 3.27 ± 3.70 and 6.34 ± 3.51 D (p = 0.01), respectively. Fig. 2 shows the mean spherical equivalent (D) measured at postoperative 1, 3, 6, 12, and 24 months. The differences in mean spherical equivalent between postoperative 1 month and 24 months was 0.84 and 2.05 D in the DSAEK and PK groups, respectively, indicative of comparably stable refractive changes for DSAEK. In addition, a hyperopic shift of 1.17 D was followed after DSAEK at 24 months.
Table 4 shows the postoperative ECD changes over the 24-month follow-up period in eyes of clear grafts in which no complications had occurred. The mean preoperative donor ECD was 2,570 ± 462 cells/mm2 in the DSAEK group and 2,720 ± 448 cells/mm2 in the PK group (Table 2). In the DSAEK group, endothelial cell loss was 25% during the first month, 31% at 6 months, and 40% at postoperative 2 years. In the PK group, endothelial cell loss was 19% during the first month, 27% at 6 months, and 61% at postoperative 2 years. Postoperative ECD was higher in the PK group up to 6 months, but this trend reversed and was higher in the DSAEK group after postoperative 6 months. Endothelial cell loss was relatively stationary in the DSAEK group and seemed to gradually plateau, whereas the PK group exhibited an abrupt decrease in ECD after 6 months. When percent cell loss was calculated by subtracting postoperative ECD at 24 months from 1 month ECD and dividing by 1 month ECD, the DSAEK group was found to have undergone a 19.96 % cell loss compared to the PK group, which had a 52.38% cell loss.
No significant difference in central corneal thickness at postoperative 24 months was found between the DSAEK and PK groups (592 ± 75 vs. 563 ± 90 µm, respectively), as shown in Table 5.
Postoperative complications
Two eyes that underwent DSAEK had graft dislocation on postoperative day 1, which was corrected with repositioning by injecting an air bubble into the AC in order to press the donor tissue against the recipient cornea. In addition, one subject in the DSAEK group had postoperative pupillary block. In the DSAEK and PK groups, two and three eyes had transient graft rejection, respectively, which was treated with intensive topical steroids and followed with close monitoring until all signs of rejection had resolved. However, there was graft failure in one eye that underwent DSAEK and two eyes that underwent PK, which all required additional keratoplasty. The main cause of graft failure found in this study was immunologic rejection. Two eyes from DSAEK and one eye from PK had high IOP during the early postoperative period, which were treated with IOP-lowering eye drops that returned the pressured to a normal range. A corneal ulcer occurred in one eye of each treatment group; however, there were no cases of endophthalmitis.
Graft survival rate
The 2-year graft survival rates for DSAEK and PK procedures used to treat bullous keratopathy were comparable. Specifically, the 2-year graft survival rates for DSAEK and PK were 93.3% and 81.8%, respectively. According to Kaplan-Meier survival analysis, the mean graft survival time after DSAEK and PK was 56 and 44 months, respectively (p = 0.344) (Fig. 3).
Discussion
This is the first study to report long-term outcomes of DSAEK and PK performed in South Korea for the same preoperative diagnosis of bullous keratopathy. The results of the present study identified a comparably stable refractive change and better visual outcome in DSAEK. According to Jun et al. [7], the mean change in refraction at an average of 5 months after in pseudophakic DSAEK is +0.71 ± 1.11 D (range, −1.75 to 3.0 D), and the overall refractive change achieved by DSAEK is +0.88 ± 1.02 D (range, −1.75 to 3.0 D), which includes a DSAEK triple surgery group. Another study by Koenig et al. [1] reported a hyperopic shift in refraction of 1.19 ± 1.32 D for patients of DSAEK not undergoing simultaneous cataract surgery. In addition, the same study indicated that refractive astigmatism, topographic astigmatism, and keratometry were not significantly different between preoperative and postoperative periods after DSAEK. In the present study, in which only bullous keratopathy was evaluated, improvement of visual acuity was achieved with only a mild tendency toward a hyperopic shift of +1.17 D and without significant induction of astigmatism after DSAEK.
All of the DSAEK and PK procedures performed in this study were carried out by an experienced surgeon, and the ECD results of the present study were consistent with data published by experienced surgeons in Western countries. Specifically, we noted an ECD of 1,548 ± 456 cells/mm2 in DSAEK group and 1,052 ± 567 cells/mm2 in PK group at postoperative 2 years. Wacker et al. [8] conducted a 5-year study of Descemet Stripping Endothelial Keratoplasty for Fuchs' endothelial corneal dystrophy, and reported an ECD at postoperative 2 and 5 years of 1,837 ± 551 cells/mm2 and 1,322 ± 487 cells/mm2, respectively. Likewise, a study by Price et al. [9] reported that at postoperative 3 years, the median ECD was 1,763 cells/mm2 following DSAEK and 1,636 cells/mm2 following PK, with a median 3-year cell loss for DSAEK and PK of 59% and 61% (p = 0.70), respectively. Another study reported that the percent endothelial cell loss was lower in eyes that underwent DSAEK compared with PK at 1 (30 ± 22% vs. 37 ± 25%, p = 0.045), 2 (36 ± 23% vs. 45 ± 33%, p = 0.018) and 3 years (39 ± 24% vs. 47 ± 28%, p = 0.022) postoperatively [10]. In our study, compared with PK, DSAEK was associated with a greater cell loss in the first 6 months, which we attributed to surgical trauma and manipulation during donor preparation and insertion, as the procedure requires skillful technique [511]. In subsequent months, however, the DSAEK group exhibited a slowing of endothelial cell loss compared to PK. These findings were consistent with a number of studies that collectively suggest that 6-month cell loss is significantly higher after EK than PK [1111213], and also that there is a high level of cell loss initially following DSAEK in the first year, but less cell loss in subsequent years [13]. In addition, according to a large prospective series by Terry et al. [11], 30% to 40% of endothelial cell loss occurs within the first year of transplantation (without significant loss between 6 months and 1 year), but appears to plateau thereafter. Likewise, the specular Microscopy ancillary study of the Cornea Donor Study [14] identified a relatively higher rate of endothelial cell loss in the early postoperative (1 year) period, but a relatively stable degree of cell loss thereafter compared to a modest increase in cell loss associated with PK.
Many corneal surgeons favor PK because of the relative ease of the procedure. However, PK carries with it a number of postoperative complications such as high and irregular astigmatic changes and prolonged visual rehabilitation, ocular surface problems, and long-term endothelial cell loss. As endothelial keratoplasty techniques have evolved, DSAEK has become a widely used method whose major advantages include stability of refraction and faster visual rehabilitation. In the present study, we found that preoperative BCVA results were similar for DSAEK and PK, while DSAEK had a 0.21 average logMAR better BCVA than PK throughout the follow-up period. In addition, visual acuity was stabilized at postoperative 1 month after DSAEK and no fluctuations in visual acuity were observed.
Despite its advantages, certain complications are unique to the DSAEK procedure. Specifically, there can be graft detachment in DSAEK as a result of the graft being held in place initially with an air bubble rather than sutures. In our study, two eyes (13.3%) had postoperative graft dislocation that was corrected by an additional injection of air into the AC. The principal cause of graft failure within 2 years after DSAEK and PK was immunologic graft rejection (incidence rate of 6.6% vs. 18.1%, respectively). The 2-year survival rate did not differ significantly between DSAEK and PK procedures performed for bullous keratopathy (93.3% vs. 81.8%, respectively, p = 0.344) and the Kaplan-Meier probabilities of survival time were not significantly different. This result was comparable to that of a previous study reporting a 3-year graft survival rate of 86% for DSAEK vs. 84% for PK (p = 0.41) in eyes mainly with pseudophakic/aphakic cornea edema [9]. Another study reported a primary graft failure rate of 3.4% for PK compared with 0.8% for DSAEK, although there was no difference in Kaplan-Meier survival probabilities for PK and DSAEK at 1 (89.7% vs. 94.1%), 2 (85.0% vs. 88.2%) and 3 years (85.0% vs. 86.5%, log-rank p = 0.671) [10].
There were some limitations to the present study. First, the subjects were not randomized, although the characteristics of the subjects were similar in that only eyes of bullous keratopathy were studied. The ideal approach to determine any statistically and, more important, clinically significant differences in clinical outcomes and graft success would be with a prospective, randomized study. A second limitation of this study was that it was difficult to directly compare astigmatism before and after the stitches were removed due to the use of selective stitch removal in some patients in the PK group, as all 11 patients had at least some remnant sutures at postoperative 2 years. Analysis of the final astigmatic outcomes of the patients in our study will require a longer follow-up period and complete removal of sutures.
In conclusion, despite a relatively large initial postoperative endothelial cell loss as well as a wide range of cell counts, most of the grafts in the study were maintained clear. To the best of our knowledge, there have been no comparative studies involving subjects of only bullous keratopathy. Therefore, this study is important in that it compared the clinical outcomes of two procedures in patients with the same diagnosis.






 XML Download
XML Download