

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Alzheimer disease (AD) is the most common form of dementia, constituting approximately 50% to 70% of all dementia cases [1]. The brains of patients with AD are notable for containing neurofibrillary tangles, which are formed by Tau protein and pair with insoluble b-amyloid (Ab) deposits called plaques. This process eventually leads to neuronal and synaptic loss [2]. In AD patients, Ab deposits and neurofibrillary tangles are present in the visual association area [3] and the subcortical visual center [4], causing a variety of visual and clinical symptoms [567].
Mild cognitive impairment (MCI) is considered a prodromal phase of AD and presents during a transitional stage between expected aging-related cognitive decline and the more serious decline of dementia [89101112]. Amnestic MCI is most likely to progress into AD and thus has attracted increased attention from various research groups [1314151617]. Despite extensive research efforts, little progress has been made in early detection of these conditions. The early stage of AD can only be diagnosed based on a combination of neuro-imaging and spinal fluid examinations, and no specific tests have been established to confirm a diagnosis of MCI. Currently, doctors must rely on the results of neurologic and psychiatric tests to determine whether MCI is the most likely cause of certain presenting symptoms [9]. Thus, it remains difficult to pathologically distinguish early AD from MCI [16]. Hinton et al. [18] were the first to report histopathologic evidence of retinal ganglion cell loss and optic nerve degeneration in patients with AD, suggesting a strong correlation between retinal degeneration and pathology of AD [17].
Optical coherence tomography (OCT) is a non-invasive imaging device used to evaluate a variety of ophthalmic conditions, including glaucoma and retinal disease. It is also able to gauge the normality of macular architecture by measuring cross-sectional retinal nerve fiber layer (RNFL) thickness and the volume and thickness of the macula with high-resolution images [1920]. OCT measurements of the retina are now able to provide new biomarkers for the detection of multiple neurodegenerative diseases, such as multiple sclerosis, Parkinson's disease, and schizophrenia [212223]. Previous reports comparing patients with AD or MCI with healthy patients indicated that those with AD or MCI have significantly reduced peripapillary RNFL thickness, as identified by OCT analysis [24252627]. There are a few studies that analyzed the relation between RNFL thickness in AD patients and in healthy normal controls and the location of thinned peripapillary RNFL. The results of the studies vary depending on whether the study included all quadrants (superior, inferior, temporal, nasal) [2528] or only the superior quadrant in their analysis. [262930]. Additionally, there are several studies analyzing the differences in RNFL between AD, MCI, and normal controls [272831].
Previous OCT studies in patients with AD and MCI demonstrated retinal nerve fiber and axonal loss with decreased peripapillary RNFL thickness [62732]. Because the macula is mainly comprised of retinal neuron cell bodies and glial cells, neuronal loss can be determined by measuring the volume of the macula on OCT [33]. Therefore, we predict that OCT-based evaluation of macular volume in this study could offer a non-invasive method for evaluating axonal loss in aging patients and in those with suspected neurodegenerative diseases [34] including both AD and MCI. Although OCT is a very easy and convenient tool, there are some factors that influence the results of RNFL thickness analysis, such as macular volume and thickness, in normal controls and MCI and AD patients. Therefore, we aimed to more meticulouly research RNFL thickness by excluding several kinds of influencing factors like age, sex, best corrected visual acuity, refractive error, and educational background.
Furthermore, in the present study, we compared the neuroanatomy, including RNFL thickness and macular thickness and volume, between healthy eyes and eyes from patients with MCI or AD. We then used these findings to evaluate the feasibility of early detection of neurodegenerative diseases with OCT.
Materials and Methods
Participants
After discussing the nature of the study with the patients, informed consent was obtained from all individual participants. This study was approved by the clinical research committee of Myongji Hospital and adhered to the principles of the Declaration of Helsinki. Thirty patients with AD and 30 patients with MCI diagnosed at the neurology department of Myongji Hospital were selected for each group. An additional 30 patients were selected for the healthy control group. All participants met the inclusion criteria and underwent diagnostic examination processes. Additionally, the cognitive state of each participant was evaluated using the Korean versions of the Mini-Mental State Examination (MMSE), Clinical Dementia Rating, and Activities of Daily Living (ADL) scales. Each group was further classified into five subgroups based on educational background. MCI was diagnosed according to the Petersen criteria [35], which include memory problems, objective memory disorders, absence of other cognitive disorders or repercussions on daily life, normal general cognitive function, and the absence of dementia. AD patients were identified based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, which requires the presence of both a memory disorder and impairment in at least one additional cognitive domain, both of which interfere with social function or ADL [36]. Brain magnetic resonance imaging or computed tomography examinations were performed in all subjects to rule out other diseases. Patients with alcohol addiction, metabolic syndrome, Parkinson disease, dementia other than AD or MCI, mental disease, hallucinations, or other ophthalmic conditions were excluded. Using the same exclusion criteria, subjects in the healthy group were selected after undergoing a neurologic examination to exclude those with cognitive disorders or dementia. Subjects in the healthy control cohort had a sex and age profile similar to those in the AD and MCI groups.
All subjects underwent ophthalmic examinations to assess best-corrected visual acuity (BCVA), eye movements, pupillary response, and intraocular pressure. They also received a slit lamp examination, visual field test, and fundoscopy. The examiners were blinded to the study aims. Participants with a BCVA of 5 / 10 or worse, refractive error >±3 diopters (D), and intraocular pressure ≥20 mmHg were excluded. Those with previously diagnosed conditions affecting OCT findings, such as macular degeneration, diabetic retinopathy, glaucoma, or vitreous hemorrhage, were also excluded. Additionally, subjects with polar cataracts according to the Lens Opacity Classification System III were excluded, as this condition could affect OCT imaging and examination outcomes. Thus, only those subjects with nuclear or cortical cataract of grade 2 or lower were included in the study.
Optical coherence tomography measurement
Cognitive testing and OCT measurements were performed on the same day. In all subjects, OCT was used to measure circumpapillary RNFL thickness, macular thickness, and volume. Eyes were dilated with 1% tropicamide solution before images were obtained with the Cirrus HD-OCT (Carl Zeiss Meditec, Dublin, CA, USA) in both eyes. Only images without a prominent involuntary saccade and with a signal strength greater than six were included. A 200 × 200 cube optic disc scan was obtained using the Cirrus HD-OCT. For image acquisition, scanning laser images were focused after the subjects were seated and properly positioned. The images were properly aligned with the optic nerve head (ONH) in the center of the scan using the iris and fundus viewpoints. Once the ONH was centered on the live scanning laser image, a 6 × 6-mm square of data was captured. The ONH analysis algorithm provided with the Cirrus HD-OCT automatically identified the borders of the optic disc and cups. Neuroretinal rim thickness, disc area, rim area, cup-to-disc ratio, vertical cup-to-disc ratio, and cup volume were automatically calculated by the Cirrus HD-OCT software. The Cirrus HD-OCT also automatically identifies the borders of the peripapillary RNFL and presents them on a circumferential RNFL thickness curve. The average superior, nasal, inferior, temporal, and 12-hour clock RNFL thickness parameters were obtained using the RNFL and ONH analysis mode of Cirrus HD-OCT.
A 512 × 128 macular cube scan was also obtained by the Cirrus HD-OCT software. Using macular thickness analysis mode, topographic surface maps were also constructed through the automated software algorithm. Central subfield thickness was identified as the average thickness in the central 1-mm subfield centered on the fovea. The inner and outer rings were divided into four quadrants with the inner ring bounded by 1- and 3-mm concentric circles and the outer ring bounded by 3- and 6-mm concentric circles. For each eye, average macular thickness, foveal thickness, inner macular (i.e., superior, nasal, inferior, temporal) thickness, outer macular (i.e., superior, nasal, inferior, temporal) thickness, and macular cube volumes were obtained. Statistical analysis was performed using the analysis of variance test, and the three groups were compared using the Tukey HSD post hoc test. The results were considered statistically significant when the p-value was less than 0.05.
Results
A total of 90 subjects were included in the study, with 30 participants in each group. The mean age was 70.93 ± 4.68 years for the healthy control group, 72.17 ± 4.98 years for the MCI group, and 73.60 ± 3.67 years for the AD group, with no statistical difference among the three groups (p = 0.08). There were 30 men and 60 women included in the study, with no statistically significant difference in sex among the three groups (p = 0.17).
BCVA was 5 / 10 or above in all three groups, and it did not significantly differ (p = 0.25). The refractive errors, which were measured with the manifest refraction (mean spherical lens equivalent), were 0.08 ± 1.69 D (right eye) and 0.47 ± 1.61 D (left eye) in the healthy group, 0.31 ± 1.82 D (right eye) and 0.21 ± 2.16 D (left eye) in the MCI group, and -0.09 ± 2.04 D (right eye) and 0.19 ± 1.80 D (left eye) in the AD group. No significant differences were noted between the three groups (p = 0.59, p = 0.71).
Educational background was evaluated by assigning a score of 0 to those who did not complete primary school, 1 to those who completed primary school only, 2 to those who completed middle school, 3 to those who finished high school, and 4 to college or university graduates. Educational background did not significantly differ among the three groups (p = 0.19). Duration of education was also not significantly different (p = 0.26). The Clinical Dementia Rating score was higher in the MCI group (0.48 ± 0.16) than in the healthy group (0.03 ± 0.12), and it was highest in the AD group (0.97 ± 0.41), with a significant difference among the three groups (p < 0.05). The ADL score was significantly lower in the AD group (18.00 ± 2.50) compared to the healthy control (20.00 ± 0.00) and MCI (20.00 ± 0.20) groups (p < 0.05, p < 0.05). The MMSE score was highest in the healthy group (27.47 ± 1.20) compared to the MCI group (24.17 ± 3.26), and it was lowest in the AD group (17.2 ± 4.29, p < 0.05).
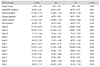
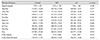
Peripapillary RNFL thickness, macular thickness and macular volume are presented and compared in Tables 1, 2, and Fig. 1. Average RNFL thickness differed significantly between the MCI and AD groups (p = 0.01), but there was no difference in average RNFL thickness between the healthy and MCI groups (p = 0.68) or between the healthy and AD groups (p = 0.09). The RNFL thickness in the superior quadrant differed significantly between the healthy and AD groups (p = 0.03). Based on measurements of each of the 12 zones, zone 11 differed significantly between the healthy and AD groups (p = 0.02), while zone 2 differed significantly between the MCI and AD groups (p = 0.03). RNFL thickness was not significantly different between the inferior, nasal, or temporal quadrants. Among the three groups, there was no difference in signal strength during the measurement of RNFL thickness (p = 0.20).
The macula became thinner and smaller in descending order from healthy controls to the MCI group to the AD group; however, these differences were not statistically significant (p = 0.23).
Discussion
Neurodegenerative diseases in adults are associated with chronic and progressive loss of structure and function of neurons. In AD, entanglement of Ab deposits and neurofibrillary tangles coupled with the loss of the cortical and hippocampal neurons results in memory loss, dementia, and accelerated brain shrinkage due to aging, which leads to serious cognitive dysfunction. Until now, there have been no established biomarkers to facilitate early diagnosis of MCI or AD [173738]. The retina shares some features with the brain. First, they share a common embryological origin, as the retina is known to branch off from the forebrain. Second, the retina and central nervous system both have similar microvascular anatomy and histologic composition. Third, its physiological features are similar to those of the blood-brain barrier. These features together make examination of the retina a useful, non-invasive, and simple means for investigating brain lesions. In particular, retinal imaging has attracted attention as a non-invasive means for evaluating the health status of axons and for measuring the effects of neuroprotective agents [39].
In most cases, the retina has no myelin, but there are cases of aberrant RNFL myelination. The retina contains axons associated with ganglion cell neurons, and the RNFL is rich in axonal tissue and has no myelin. This makes it a potentially useful biomarker of axonal loss in the central nerve system, such as in multiple sclerosis [40]. There are several reports that RNFL thickness is significantly decreased in AD patients compared to healthy controls [242526272830414243]. He et al. [39] also reported that RNFL thickness is significantly decreased in all quadrants in AD patients. Other reports, however, indicate that RNFL thickness differs significantly in the superior [2641] and inferior quadrants [28]. In the present study, we found the RNFL thickness was significantly decreased in the superior quadrant in AD patients compared to healthy controls (p = 0.03). The average RNFL thickness was significantly decreased in the AD group compared to the MCI group (p = 0.01).
There are also studies that assess RNFL differences between AD, MCI, and normal controls. A large proportion of patients with amnesic MCI ultimately develop AD, but the conversion rate varies depending on the diagnosis category [42]. It has been shown that RNFL thickness in the superior quadrant gradually decreased from MCI to increasing severity of AD compared to controls [31]. Paquet et al. [27] reported that the RNFL is thinner in patients with MCI and AD compared with controls, based on OCT. Kesler et al. [28] showed that, in both AD and MCI groups, inferior RNFL thickness decreased compared to the control group, and that the superior RNFL thickness decreased in the AD group compared to the control group. Unlike the findings of these studies, we found that average RNFL thickness was slightly increased in the MCI group compared to the healthy cohort. A potential explanation for this finding could be that gliosis occurs prior to the loss of neurons, which produces an initial thickening of the RNFL, followed by neuron loss and tissue thinning. This process has been shown in a number of degenerative eye diseases. It is possible that gliosis leads to lack of difference or an initial paradoxical increase in RNFL thickness on OCT, and that only AD patients with axonal degeneration show appreciable RNFL thinning on OCT. Further analysis and research are needed to investigate these findings.
Age-related thinning of the superior peripapillary RNFL in the eyes of healthy subjects has also been reported based on OCT analysis [44]. Such a decrease in RNFL thickness was significantly greater in the MCI and AD patient groups when all subjects were stratified by age [44].
Anatomically, axons from the superior retina project via the parietal portion of the optic radiation to the cuneal gyrus of the primary visual cortex, whereas axons from the inferior retina project to the lingual gyrus. In a histopathological study of cortical damage in AD, Armstrong found a greater density of senile plaques and neurofibrillary tangles in the cuneal gyrus than in the lingual gyrus, providing a potential explanation for the predominantly superior RNFL thinning that occurs in AD.
Another study demonstrated a significant decline in overall macular volume in AD patients compared to controls. This decrease in volume was shown to correlate with MMSE score [25]. The present study found significant difference among the three groups in terms of MMSE score and ADL, but no significant difference was seen in macular thickness or volume. Furthermore, MCI patients had the greatest macular volume, followed by controls and then AD patients [43]. Additional studies about the relationship between RNFL and cognitive dysfunction showed that patients who progressed from MCI to AD had a greater reduction of RNFL thickness than patients with stable AD or MCI [45]. It was also shown that nasal quadrant RNFL thickness was positively correlated with episodic memory scores in patients with normal cognition, while inferior quadrant RNFL thickness was inversely correlated with episodic memory scores in MCI patients [46].
As a unique central nerve system structure composed of axons and glia with no myelin, the retina is ideal for evaluating axonal and neuronal degeneration based on RNFL and macular thickness on OCT. The RNFL is comprised of axons from the retinal ganglion that converge onto the optic disc head. Using peripapillary RNFL thickness, one can evaluate the health status of the axon and the extent of axonal loss [40]. Furthermore, because macular volume is determined by the retinal ganglion cell bodies, photoreceptors, and other cell types, macular volume measurements can provide information regarding the status of the neurons and neuronal loss [21]. In this study, although the differences of macular thickness and volume were not statistically significant, macular thickness and volume decreased in the MCI and AD groups compared to the healthy controls. In another study of similar design, retinal degeneration in AD and MCI patients resulted in decreased thickness of the RNFL and reduced macular volume in AD and MCI patients [2]. While these results differed from ours, there were subtle distinctions between the two studies, like the number of participants and the statistical methods used. Specifically, our study controlled for interference factors originating from age differences by ensuring that all subjects were in same age group, regardless of whether they belonged to the healthy cohort or the MCI or AD group. Additionally we considered sex, best corrected visual acuity, refractive error, and educational background as potential influencing factors, and such considerations are reflected in the results.
In this study, we analyzed the differences in peripapillary RNFL thickness and macular sector thickness between AD, MCI, and control eyes. The major limitations of this study include the relatively small number of subjects involved and the lack of follow-up. Also, this study is also limited in its evaluation of macular layer thickness, as segmental analysis of the ganglion cell complex is required. Some strengths of this study are its strict control over the number of subjects and its strict inclusion and exclusion criteria, which allowed us to generate accurate and well-controlled results. We also used spectral-domain OCT, which has better resolution than time-domain OCT.
In conclusion, measuring the average RNFL thickness might help to differentiate MCI from AD and to differentiate AD from health patients based on RNFL thickness in the superior quadrant of the peripapillary region. Ultimately, we determined that RNFL thickness was a useful discriminator for these diseases, but that macular thickness was not.
Despite the limitations mentioned above, our findings suggest that OCT measurements can be useful for diagnosing early AD and for monitoring subsequent changes in the retina in AD and MCI patients. Further studies are needed to investigate the correlation between the specific retinal sublayer identified on OCT and the neurological pathology in AD. A better designed imaging study should be implemented to determine the relationship between decreased thickness in the RNFL and the central retina and progression of MCI and AD. In addition, more in-depth and long-term studies are needed to identify potential biomarkers of AD.

 XML Download
XML Download