

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dry eye syndrome is a multifactorial disease of tears and the ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability, with potential damage to the ocular surface [1]. The aqueous-deficient type is characterized by reduced lacrimal tear secretion and volume, resulting in symptoms of dry eye. Three percent diquafosol tetrasodium ophthalmic solution (Diquas ophthalmic solution 3%; Santen Pharmaceutical, Osaka, Japan) acts as a P2Y2 purinergic receptor agonist, stimulating both fluid secretion from conjunctival epithelial cells and mucin secretion from conjunctival goblet cells directly on the ocular surface [2]. Consequently, diquafosol can rehydrate the ocular surface independent of tear secretion from the lacrimal glands. This action stabilizes tear film on the ocular surface and provides clinical improvement for symptoms of dry eye [34].
Anterior segment optical coherence tomography (OCT) is a relatively new noncontact method of imaging the anterior segment that can provide detailed information on the status of the tear meniscus. Another benefit of OCT is that it allows noninvasive visualization of the tear meniscus without requiring the use of dyes [5]. Initial anterior segment-OCT imaging devices such as the Visante OCT (Carl Zeiss Meditec, Dublin, CA, USA) and slit-lamp OCT (Heidelberg Engineering, Dossenheim, Germany) employ time-domain technology, and have been shown to be effective for measurement of tear meniscus [678]. Spectral-domain OCT (SD-OCT) devices have recently become widely available, offering significant advantages over previous time-domain OCT devices, including higher speed, greater sensitivity, and higher resolution [9].
In this study, using SD-OCT, we evaluated changes in tear volume after the instillation of a drop of 3% diquafosol ophthalmic solution or normal saline in patients with dry eye syndrome.
Materials and Methods
Approval was obtained from the institutional review board of Konyang University Kim's Eye Hospital before the initiation of the study. Research was conducted in compliance with the Declaration of Helsinki, and prior written informed consent was obtained from all subjects after an explanation of the nature of the study and possible consequences associated with participation.
Sixty eyes from 30 patients (eight men and 22 women) with mild to moderate dry eye syndrome were included. Patients were diagnosed based on the following criteria: tear film break-up time (TBUT) ≤5 seconds and corneal staining score by Oxford schema ≥1 [10]. Exclusion criteria were as follows: systemic disease related to dry eye syndrome (e.g., Sjögren's syndrome), acute ocular infection or inflammation not associated with dry eye, drug toxicity, contact lens wearer, ocular allergy, recent ocular surgery (less than 3 months), conjunctivochalasis, and eyelid or eyelash disorder.
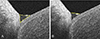
We used anterior segment SD-OCT (Cirrus 5000, Carl Zeiss Meditec) with a mean value of vertical 5-line raster scan images at the midline of the lower lid margin (Fig. 1). Tear meniscus area (TMA) and tear meniscus height (TMH) were measured with images acquired from the OCT using the National Institutes of Health's image-analysis software (ImageJ 1.44p; National Institutes of Health, Bethesda, MD, USA) (Fig. 2A, 2B). TMA and TMH were measured at baseline, 5 minutes, 10 minutes, and 30 minutes after instillation of a drop of diquafosol in one eye and normal saline in the other eye (Fig. 3). Solutions were assigned randomly to each eye using a table of random sampling numbers. All examinations were performed by the same blinded examiner.
Changes in ocular surface disease index (OSDI) score, TBUT, corneal staining score by Oxford schema, and meibomian expressibility were evaluated at baseline, 1 week, and 1 month after the use of diquafosol 6 times a day. Meibomian expressibility was measured using the method reported by Pflugfelder et al. [11]: compressing the five orifices of the meibomian glands of the lower lid with a finger, and counting the glands expressing meibum (grade 0, 5 glands; grade 1, 3–4 glands; grade 2, 1–2 glands; grade 3, 0 gland). Results were analyzed with a paired t-test using SPSS software ver. 12.0 (SPSS Inc., Chicago, IL, USA).
Results
This study included 60 eyes of 30 subjects (mean age, 29.3 years; 8 men and 22 women). In eyes that received diquafosol, tear volume was increased at 5 minutes and 10 minutes compared to baseline. Mean TMA was 13,305.53 ± 1,604.78 µm2 at baseline, 17,674.26 ± 2,110.34 µm2 at 5 minutes (p < 0.001), 19,144.52 ± 1,981.22 µm2 at 10 minutes (p = 0.003), and 15,566.55 ± 2,041.95 µm2 at 30 minutes (p = 0.189). Mean TMH was 227.36 ± 15.08 µm at baseline, 265.13 ± 16.22 µm at 5 minutes (p < 0.001), 268.54 ± 15.17 µm at 10 minutes (p < 0.001), and 240.57 ± 15.48 µm at 30 minutes (p < 0.339). In eyes that received normal saline, tear volume was slightly decreased at 5 minutes and 30 minutes, but this difference was not statistically significant. Tear volume of the eyes that received diquafosol was higher than that seen in saline-applied control eyes at 5, 10, and 30 minutes (TMA: p = 0.016, p < 0.001, and p = 0.023; TMH: p = 0.004, p < 0.001, and p = 0.023, respectively) (Fig. 4).
Tear volume after the use of diquafosol six times a day was not changed at 1 week and at 1 month, but tear volume was increased at 10 minutes after the instillation of a drop of diquafosol at each visit (Fig. 5). OSDI score, TBUT, and Oxford cornea stain score improved significantly at 1 week and 1 month after the use of diquafosol, but meibomian expressibility was not changed (Fig. 6A-6D).
Discussion
Slit lamp examination, fluorescein dye staining, TBUT, and the Schirmer test are the traditional diagnostic approaches for dry eye syndrome. However, there have been concerns about the low diagnostic efficiency and reproducibility of these tests [12]. OCT has the advantage of being a noninvasive in vivo technique for quantitative measurement of tear film and tear meniscus that does not require ocular surface contact or dye instillation [1314].
Yokoi et al. [4] reported increased tear volume after the instillation of a diquafosol ophthalmic solution, using video meniscometry. However, reflective video meniscometry is not a commonly available method in clinical settings [15]. Koh et al. [3] reported the preliminary long-term efficacy of diquafosol for aqueous-deficient dry eye [3]. They found that diquafosol reduced dry eye symptoms and ocular surface staining, and increased TBUT and TMH measured by swept source-OCT (SS-1000; Tomey, Nagoya, Japan).
OCT is a non-invasive optical imaging technique that is clinically utilized for acquiring high-resolution, cross-sectional images of the retina, optic nerve, and anterior segment, aiding in the diagnosis and monitoring of various ocular diseases. Conventional time-domain OCT employs a mechanical scanning reference arm and sequentially measures the echo time delays. In contrast, newer generation spectral or Fourier domain OCT uses a stationary reference arm to obtain an interference spectrum, which then undergoes Fourier transformation to allow for the simultaneous measurement of all light echo time delays. SD-OCT technology further improves on the time-domain systems, allowing the performance of up to 27,000 axial scans per second. The increased axial scan rate results in an approximately 50 times faster data acquisition in practice. As a result, this new technology significantly improves system speed and sensitivity [1617].
To date, most tear meniscus studies measured TMA or TMH using Fourier-domain OCT (RTVue-100; Optovue, Fremont, CA, USA) [181920] or time-domain OCT [67]. RTVue offers more anterior than posterior segment OCT features. In the current study, we used SD-OCT (Cirrus 5000, Carl Zeiss Meditec), which is the most commonly used model, for the evaluation of tear meniscus volume in patients with dry eye syndrome and we were able to quantify tear meniscus quickly and accurately.
In this study, we demonstrated the facilitation of tear secretion by a 3% diquafosol ophthalmic solution using anterior segment SD-OCT. Tear volume of the eyes receiving diquafosol was increased at 5 and 10 minutes compared to baseline, and was significantly higher than in saline instilled control eyes at 5, 10, and 30 minutes.
A previous report found that the increase in tear meniscus lasted for only 5 minutes after artificial tear instillation, and for only 10 minutes after 0.1% sodium hyaluronate instillation [21]. Another study on the topical instillation of 0.5% carboxymethylcellulose in healthy eyes also reported that meniscus height and cross-sectional area returned to baseline levels at 5 minutes after instillation [22]. According to our findings, 3% diquafosol ophthalmic solution sustained the increase in tear volume for 10 minutes compared to baseline.
Our results showed a statistically significant improvement in OSDI, TBUT, and Oxford cornea staining scores after 1 week and 1 month of daily instillation of diquafosol, but meibomian expressibility was not improved. In this study, meibomian expressibility was measured with a method reported by Pflugfelder et al. [11] that used digital pressure. There are various means for measuring meibomian expressibility, and more recently instruments that can standardize the pressure (meibomian gland evaluator; TearScience Inc., Morrisville, NC, USA) have been developed. With this small handheld instrument, a defined pressure is applied to the lateral, middle, and nasal third of the lower eyelid, and the number of secreting glands is counted [23]. Further studies implementing such tools might be necessary to obtain more objective and accurate results.
This study has several limitations regarding placebo drug use. Because 3% diquafosol has higher viscosity than normal saline, OCT variables might be influenced by its different viscosity and hydrophilicity. We recognized this problem when we designed the study. However, the proper drug vehicle, with identical constituents except the active ingredient (3% diquafosol), was not available. Therefore, we had to conduct this study with normal saline. Further study comparing the effects of diquafosol with an appropriate placebo drug might be necessary.
In conclusion, tear meniscus evaluation by anterior segment SD-OCT demonstrated the enhancement of aqueous tear secretion by 3% diquafosol ophthalmic solution. Therefore, 3% diquafosol might be helpful in the treatment of dry eye syndrome, particularly in the aqueous-deficient type.





 XML Download
XML Download