

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Central retinal artery occlusion (CRAO) is an acute vascular event that causes painless and sudden visual loss in the affected eye [1]. It develops when the central retinal artery is occluded with emboli, which results in a retinal infarction (similar to a cerebral infarction) [1]. The incidence of CRAO is low, approximately 5 per 100,000 person-years in people over 50 years of age [2]. Individuals with cardiovascular disease are at a higher risk for developing CRAO [3]. Iatrogenic CRAO is rare but can occur during cosmetic facial filler injection, retrobulbar anesthesia, embolization treatment, and head and neck drug injection [4567]. Retrobulbar anesthesia has been used for years in intraocular surgery. Complications related to this procedure (retrobulbar hemorrhage, direct optic nerve trauma, scleral perforation, and CRAO) are rare, but may lead to dramatic and permanent vision loss if they do occur [89].
Despite the occurrence of numerous CRAOs following intraocular surgery with retrobulbar anesthesia [81011121314], clinical features of this condition, including detailed ophthalmologic evaluations, cerebrovascular imaging, and visual outcomes after treatment, are not well documented. We report a case series of 5 patients who developed CRAO after uneventful intraocular surgery with retrobulbar anesthesia.
Materials and Methods
This study was approved by the institutional review board of Seoul National University Bundang Hospital. Electronic medical records of consecutive patients who visited Seoul National University Bundang Hospital between November 2008 and August 2014 were reviewed for study eligibility. Inclusion criteria included acute non-arteritic CRAO that was newly diagnosed with fundus photography and/or fluorescein angiography within 1 day of intraocular surgery. Following the diagnosis of CRAO, some patients underwent super-selective intra-arterial thrombolysis with urokinase and tirofiban within 24 hours of symptom onset as a standard-of-care procedure. Informed consent was obtained from patients for this procedure.
Data collected included ocular and/or systemic disease presence, demographics, preoperative ocular abnormalities, anesthesia technique (i.e., anesthetic agent, anesthetic dose, needle type), treatment type, initial and final best-corrected visual acuity, and follow-up duration. Each patient underwent a complete ophthalmologic evaluation, including spectral domain optical coherence tomography, fluorescein angiography, and electroretinography. Systemic risk factors were also assessed and, in patients who underwent intra-arterial thrombolysis, cerebrovascular status was evaluated using transfemoral cerebral angiography.
Results
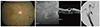
A total of 5 patients (2 men [40%] and 3 women [60%]) met all inclusion criteria (Figs. 1,2,3,4,5). Patient demographics and clinical characteristics are summarized in Table 1. A total of 3 (60%) patients had isolated CRAO and 2 (40%) patients had CRAO with ophthalmic artery occlusion. The mean patient age was 67.0 ± 8.2 years (range, 53 to 72 years). All patients had one or more vascular risk factor, including hypertension, diabetes, prior cerebral infarction, myocardial infarction, and/or carotid artery stenosis. All patients presented with acute visual disturbance noted when they removed their eye patches 1 day after uneventful intraocular surgery. There were 2 (40%) patients who underwent cataract surgery (phacoemulsification and posterior chamber intraocular lens implantation) and 3 (60%) patients who underwent vitrectomy (1 patient with air). Patients were managed with observation (1 case), anterior chamber paracentesis (1 case), or intra-arterial thrombolysis (3 cases). In the 3 patients who underwent intra-arterial thrombolysis, transfemoral cerebral angiography revealed ophthalmic artery stenosis in 1 case, internal carotid and ophthalmic artery stenosis in 1 case, and no steno-occlusive or remarkable lesions in 1 case. Mean follow-up duration was 1,139.4 ± 710.1 days (range, 4 to 1,807 days) and final visual outcome was poor in all patients. At the last follow-up visit, best-corrected visual acuity was no light perception in 2 eyes, light perception in 1 eye, and the ability to count fingers in 2 eyes.
Discussion
Despite various modifications in retrobulbar anesthesia methods, blindly inserting a needle into the retrobulbar space is still necessary and can result in vision-threatening complications [15]. Many previous articles have reported iatrogenic CRAO following retrobulbar anesthesia (Table 2) [5810111214161718]. In these reports, 10 of 17 cases occurred following intraocular surgery (cataract surgery or vitrectomy). Because no CRAOs were observed following intraocular surgery without retrobulbar anesthesia, the main cause of CRAO is thought to be retrobulbar anesthesia and not the intraocular surgery itself. As in the 5 cases reported here, the majority of previously reported cases had a poor visual outcome.
The mechanism of iatrogenic CRAO associated with retrobulbar anesthesia is not well understood. Klein et al. [5] suggested that direct central retinal artery trauma and pharmacologic and/or compressive anesthetic agent effects resulted in retinal vascular occlusions following retrobulbar anesthesia. Morgan et al. [13] also described mechanisms of vascular obstructions associated with retrobulbar anesthesia. They believe that trauma of and partial anesthetic injection into the central retinal artery resulted in embolization of the retinal circulation. Additionally, injection of anesthetic agents into the optic nerve sheath may occlude both the central retinal artery and vein [9121319]. Because central retinal vein occlusion was not observed in any of our patients, we consider optic nerve sheath hematoma to be an unlikely cause of CRAO in our patients.
Horven [20] and Vinerovsky et al. [21] documented that retrobulbar and peribulbar injection of a nesthetic agent causes vasoconstriction of the ophthalmic artery and a subsequent reduction in ocular blood flow. We recently suggested retrograde embolic propagation through collateral ophthalmic artery vessels as a mechanism for CRAO development following cosmetic facial filler injection [7]. Although injection agents and sites were different than those examined in this study, this phenomenon may still underlie CRAO development following retrobulbar anesthesia. Sharp needles were used in 4 of our 5 CRAO patients to deliver anesthetic, supporting the notion that direct injury to the ophthalmic artery or its collaterals can result in CRAO. In 4 out of the 17 previously reported cases (Table 2), retrobulbar hemorrhage or optic nerve sheath hematoma were observed. Although the cause of CRAO in these 4 cases remains unclear, and direct central retinal artery compression cannot be ruled out, injury to the central retinal artery or its branches may have caused the formation of vascular emboli and CRAO.
It is known that CRAO is associated with vascular risk factors, including hypertension, cardiac disease, carotid artery disease, and cerebral infarction [3]. Given that all of our patients (Table 1) and most previously reported patients (Table 2) had one or more vascular risk factor, we conclude that pre-existing cerebrovascular disease may increase the risk of developing iatrogenic CRAO following the administration of retrobulbar anesthesia.
This study is limited by the retrospective design and small sample size. However, to the best of our knowledge, the 5 cases included here make up the largest cohort of patients with retrobulbar anesthesia-associated CRAO in Korea. We hope that our detailed description of clinical features and visual outcomes will be helpful to ocular surgeons. In conclusion, iatrogenic CRAO is a vision-threatening complication associated with retrobulbar anesthesia administered for intraocular surgery. Patients who are elderly and have one or more vascular risk factor may be at an increased risk for this complication. Although rare, patients should be educated on iatrogenic CRAO prior to intraocular surgery with retrobulbar anesthesia. Precautionary measures (e.g., using a blunt needle) should be implemented to minimize the risk of iatrogenic CRAO, particularly in patients with vascular risk factors.






 XML Download
XML Download