

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Nasal packing after dacryocystorhinostomy (DCR) is an optional procedure to prevent nasal bleeding [1,2]. Although improvements in surgical technique have reduced the need for this practice, nasal packing is still needed more for Asians than for Caucasians due to anatomical differences. Compared to Caucasians, Asians have a thicker lacrimal bone, a thicker frontal process of the maxilla, and a narrower nasal passage [3-5]. In addition, the proportion of the maxilla to the lacrimal bone in the lacrimal sac fossa is greater than in Caucasians [4]. Such anatomical differences make osteotomy more difficult and prone to nasal bleeding in Asians when performing DCR. Postoperative nasal bleeding is unpleasant for patients and can be severe in certain cases [2,6]. It can potentially affect the mucosal healing process and can cause fibrosis and induce scarring at the newly formed rhinostomy site, all of which could result in an impairment of ostial patency [7]. Therefore, the minimization of intra- and postoperative bleeding is important to consider in an attempt to achieve successful surgical results.
The effects of nasal packing are not limited to hemostasis, as it also directly affects wound healing [8-14]. In the field of endoscopic sinus surgery, a number of papers have investigated whether or not nasal packing, both in general and in regard to the type used, affected nasal mucosal re-epitheliazation, fibrous tissue proliferation, granulation, and synechiae formation [8,11-13]. More recently, the effects of nasal packing materials after DCR have started to draw attention [10], but there are no well-established conclusions due to the scarcity of reports. Furthermore, the lack of standardization in the measurement of DCR surgical outcomes makes it difficult to compare and interpret the results of previous studies [15].
Packing materials are broadly divided into non-absorbable and absorbable materials. Non-absorbable materials include Vaseline gauze strips and Merocel, which inhibit bleeding through a compression mechanism [8]. Absorbable materials such as Gelfoam [1,9] and MeroGel [10] have been reported to be successful as packing materials after DCR. Nasopore, a bioresorbable dressing for the nasal cavity, is composed of fully synthetic biodegradable, fragmentable foam that absorbs fluids while supporting and providing pressure against the surrounding tissue. As such, it could potentially prevent undesired postoperative adhesions [13].
To investigate the effects of postoperative packing with Nasopore, we placed Nasopore at the anastomosis site of newly formed anterior mucosal flaps. Patients who had their nasal cavities packed with Merocel packing were recruited as a control group. Merocel, due to its non-absorbable character, is supposed to be removed within 2 to 3 days after its application.
We investigated the degree of postoperative re-bleeding and the level of patient discomfort and compared the anatomical and functional success rate 3 months post-surgery between Nasopore and Merocel. To our knowledge, this is the first report to investigate the effect of Nasopore on the surgical outcome of DCR.
Materials and Methods
Patients
A review of the medical records of patients with primary acquired nasolacrimal duct obstruction (NLDO) who underwent external DCR (Ex-DCR) or endonasal endoscopic DCR (EES-DCR) by a single surgeon (JSY) at Severance Hospital from January 2008 to December 2010 was retrospectively performed. Patients with secondary NLDO, such as that caused by trauma, tumor, or dacryocystitis, were excluded from the study. Patients with less than 3 months of follow-up were also excluded. Patient histories of hypertension, diabetes, the presence of distal canalicular stenosis, and aspirin use were investigated. If a patient was on blood thinners, they were discontinued around perioperative periods; for example, aspirin and non-steroidal anti-inflammatory drugs were discontinued at 1 week and Coumadin at 4 days.
In cases of Ex-DCR, the type of the newly formed anterior mucosal flap (e.g., anchoring between the lacrimal sac and the nasal mucosa or between the lacrimal sac and the periosteum) was investigated. A narrow nasal cavity was defined preoperatively and during surgery by the presence of nasal septal hypertrophy or septal deviation that made it difficult to observe the DCR opening site above the neck of the middle turbinate. For each patient, Nasopore (lactide caprolactone co-polyesters; Polyganics, Rozenburglaan, Groningen, The Netherlands) and Merocel (polyvinyl alcohol; Medtronic Xomed, Jacksonville, FL, USA) were randomly selected and applied. The surgeon preferred Ex-DCR for patients with a narrow nasal cavity or severe septal deviation, whereas EES-DCR was preferred for patients with more concerns about facial scarring.
Written informed consent was obtained from each patient. This research adhered to the tenets of the Declaration of Helsinki and was approved by the international review board at Severance Hospital of Yonsei University.
Surgical technique
The surgery was performed under general anesthesia. In both Ex-DCR and EES-DCR, an infratrochlear block using 2% xylocaine (AstraZeneca, Wilmington, DE, USA) and preoperative packing of bosmine-soaked gauze into the nasal cavity was performed. For Ex-DCR, 2% xylocaine was also injected along the skin incision marking for hemostasis. For EES-DCR, an additional injection of 2% xylocaine into the lateral nasal wall was performed.
Ex-DCR was performed in a standardized fashion [16]. The lacrimal sac and the nasal mucosa from the osteotomy margin were used to make an anterior flap. The posterior flap was not fashioned in all surgeries. After making a pre-placed suture of nasal mucosa, bicanalicular silicone intubation was performed (Fig. 1A). Four centimeter pieces of Nasopore were soaked in a gentamycin solution, squeezed, cut into three pieces, and packed one by one at the anastomosis site as deep as the common canaliculi opening to maximize the pressure and tenting effect on the lacrimal sac (Fig. 1B). Then a preplaced suture of 6-0 Vicryl was passed through the other edge of the sac flap to complete the anterior flap (Fig. 1C). For patients in whom a nasal mucosal flap could not be made, the anterior edge of the lacrimal sac flap was sutured onto the periosteum of the osteotomy site lip. For patients to whom Merocel was applied, Merocel was cut into two pieces and placed into the entire nasal cavity after skin wound closure. Especially in patients with a narrow nasal cavity, the packing material maintained the nasal wound separated from the nasal septum (Fig. 1D).
EES-DCR was also performed following standard methods [16]. The lacrimal sac was tented with a probe, incised with a sickle knife to make the posterior lacrimal sac, and flattened into the lateral nasal mucosal wall. Nasopore was packed in the same manner as in Ex-DCR at the anastomosis site.
Patients were instructed to instill topical antibiotics and steroid eye drops four times a day and to use a mometasone furoate nasal spray twice a day after the removal of packing. In patients with Nasopore packing, the packing was partially suctioned out at 1 week postoperatively, leaving a portion of the packing around the anastomosis site to be degraded naturally. The Merocel packing was removed 2 to 3 days after surgery. The follow-up visits were at 1, 2, 4, 8, and 12 weeks postoperatively. At every visit, nasal wounds were examined by endoscope and cleaned with suction and forceps. Whenever granuloma at the nasal wound was observed, it was removed and the wound was more closely examined within shorter follow-up periods. All the patients were instructed to use a steroid nasal spray and irrigate their nasal cavity using normal saline, postoperatively.
Outcome measurement
The degree of nasal re-bleeding was assessed during postoperative week 1, meaning that all of the bleeding within a week of surgery as well as the bleeding associated with the removal of packing material was defined as re-bleeding. Bleeding was categorized into three grades: no bleeding event, re-bleeding occurred but stopped spontaneously within one hour, or re-bleeding occurred and re-packing was necessary to stop bleeding for a few hours. The degree of subjective discomfort for the 2 days during which packing materials were still inside the nasal wound was surveyed. The patients were asked to rate their discomfort degree as mild discomfort, moderate, or severe.
The postoperative success rate was evaluated 3 months after surgery. The success rate was assessed according to anatomical success and functional success separately (Table 1). Success was scored in a binary pattern. Anatomical success was assessed with a lacrimal syringe test and with examination of the passage of fluorescein dye (F-dye) using a nasal endoscope. Results were categorized as either 'well passed,' 'partially passed,' or 'not passed,' which were recorded as success or fail, respectively. F-dye was instilled into the lower conjunctival sac, and the time until it was visible at the nasal ostium under endoscopic nasal exam was measured. The surgery was defined as a success if the dye was visible at the nasal ostium with an endoscope within 10 seconds, whereas the surgery was defined as a functional failure when the dye was not visible within 10 seconds. In addition, using a nasal endoscope, any granulations, synechiae, or membrane formations within 1 to 2 mm of the nasal ostium were identified.
Functional success was evaluated by subjective ocular symptoms. The degree of subjective epiphora was assessed by the Munk score [17]. A Munk score of 0 to 1 defined the surgery as a functional success, while a Munk score of 2 to 5 defined the surgery as a functional failure.
Data analysis and statistics
All statistical analysis was performed with the SPSS ver. 19.0 (SPSS Inc., Chicago, IL, USA), and a p-value of less than 0.05 was considered statistically significant. To compare the primary data between the two groups, we used the independent t-test and the Pearson's chi-square test. For the comparison of the degree of postoperative re-bleeding and the level of patient discomfort, as well as the surgical success rates between groups, a Pearson's chi-square and Fischer exact test were used.
Results
A total of 77 patients (101 eyes) were included in this study. Of the 101 eyes, 30 were packed with Nasopore, while 71 were packed with Merocel. The demographics and clinical data of the patients are shown in Table 2. There were no statistically significant differences between the two groups in age, sex ratio, the ratio of right-eye surgery to left-eye surgery, the ratio of Ex-DCR to EES-DCR, and the cases with a narrow nasal cavity. However, there was a larger proportion of patients with preoperative canalicular stenosis in the Nasopore group than in Merocel group (p = 0.042, Pearson's chi-square test) (Table 2).
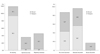
The packing material after DCR was associated with the degree of re-bleeding and the level of patient discomfort. The nasopore group showed significantly better results than the Merocel group (p = 0.000, 0.039, respectively; Pearson's chi-square test) (Table 3 and Fig. 2). Accordingly, 93.3% of the patients with Nasopore showed no bleeding event during one week after surgery, whereas 42.3% of the patients with Merocel required nasal repacking to stop bleeding at the time of Merocel removal (Fig. 2). All of the re-bleeding events in patients with Merocel occurred at the time of packing removal. No patient with Nasopore described severe discomfort, whereas 16.9% of the patients with Merocel felt severe discomfort (Fig. 2). No differences were observed regarding the anatomical and functional success rate between the Nasopore and Merocel groups (all p > 0.05) (Table 4).
Additionally, we did a sub-analysis by comparing parameters such as re-bleeding, discomfort, and surgical success rate of each packing material in groups categorized by two surgical types (Ex-DCR and EES-DCR). In both surgical groups, cases with Nasopore had significantly less re-bleeding than with Merocel (p < 0.001). In cases using Nasopore, re-packing was done in 1 / 19 eyes (5.3%) in Ex-DCR and 0 / 11 eyes (0%) in EES-DCR, whereas in cases using Merocel, re-packing was done in 25 / 55 eyes (45.5%) in Ex-DCR and 5 / 16 eyes (31.3%) in EES-DCR. However, the degrees of discomfort, surgical success rate, or postoperative nasal findings were not different according to the packing materials in each surgical group (data not shown).
Discussion
The most common causes of DCR failure are having a small bony ostium that is located improperly, scarring at the rhinostomy site, and ostial obstruction caused by granulation or fibrosis [7,9]. To ensure anatomical and functional success and in order to prevent the collapse of newly formed mucosal flaps and unwanted fibrotic closure, it is important to create a bony ostium of the proper size, reduce the intra- and postoperative bleeding, and to make the canalicular opening wider toward the nasal opening.
Several techniques for making a wider canalicular opening have been reported, including anchoring of the anterior lacrimal sac flap to the periosteum [18], lacrimal diaphragm and periosteum suturation [19], bicanalicular double silicone intubation [20], the sleeve technique (i.e., sustaining the sleeve at the opening site) [21], and the use of mitomycin C [22]. It is thought that anchoring the anterior flap to the periosteum and the sleeve technique might especially help prevent the newly formed anterior mucosal flap from collapsing because the sac flaps are physically tented [18,21]. We expected to achieve a similar mechanical tenting effect by placing the absorbable packing materials at the site of the newly-formed anastomosis before the suturing of the anterior flaps (Fig. 1).
Nasopore consists of a biologically inert foam and has a highly interconnected porous structure that is highly absorbent and can absorb up to 25 times its weight. It is believed to provide gentle compression and offer sufficient wound support during the critical healing period through the absorption of nasal fluids and blood [13]. Also, Nasopore can accelerate wound healing by providing a wet dressing environment. It can be more helpful for wound healing, especially in EES-DCR cases more so than in Ex-DCR cases. The former is associated with wound healing that takes about two or more weeks by secondary intension healing, whereas the latter is associated with primary intension healing [23]. Maintaining a large mucosal opening with Nasopore for approximately one week is expected to help prevent the adhesion of the anterior mucosal flaps by both a mechanical volume effect and the absorption of blood. Although we had hoped that this would lead to better results in terms of ostial patency, the difference in surgical success between Nasopore and Merocel did not prove statistical significance in the present study. We believe that this is probably due to the high functional success rates of external DCR, which is greater than 90% in both groups, or due to a small sample size. In the present study, we did a sub-analysis by comparing parameters such as re-bleeding, discomfort, and surgical success rate of each packing material in groups categorized by two surgical types (Ex-DCR and EES-DCR). In both surgical groups, cases with Nasopore had significantly less re-bleeding than with Merocel.
However, the degree of discomfort, surgical success rate, and postoperative nasal findings did not differ according to the packing materials in each surgical group. Considering the results of combined Ex- and EES-DCR (101 eyes), which showed that Nasopore had significantly less discomfort than Merocel (p = 0.039, Pearson's chi-square test), this is probably due to the decreased sample size resulting from sub-grouping.
In several previous reports on the effects of absorbable packing material on postoperative bleeding, discomfort and nasal wound healing showed contrary results. Berlucchi et al. [12] reported that absorbable packing material showed a lower proportion of nasal adhesion and improvement of endoscopic nasal findings such as re-epithelialization, granulation, and the appearance of mucosa of the nasal cavities after endoscopic sinus surgery, compared to non-absorbable packing material. However, Wang et al. [8] reported that Nasopore packing showed a trend toward causing granulation tissue formation during the early stages of wound healing and a higher incidence of major bleeding, which led the authors to reason that Nasopore provided less compression onto mucosa. In another report by Shoman et al. [13], there was no significant difference between Nasopore and Merocel in regard to the risk of bleeding or patient discomfort, which contradicted our results. However, the Merocel packing used in this study was placed in a vinyl glove finger, so we assume that use of a vinyl glove might reduce the potential damage to the nasal mucosa from the pressure of the packing or from the trauma of packing removal. In addition, these reports involved cases of endoscopic sinus surgery, and therefore it is difficult to compare the results from previous reports with our results.
There is a scarcity of reports involving cases of DCR. Wu et al. [10] reported that another absorbable pack, Merogel, an esterified derivative of hyaluronan, was associated with a larger number of healed ostium with a lining of intact epithelial mucosa, less formation of scarring, and a greater success rate of ostial patency, compared to those in the non-packed group after endoscopic DCR. In the present study, we compared the degree of postoperative re-bleeding, the level of patient discomfort, and the anatomical and functional success rate of external DCR between absorbable and non-absorbable packing materials. We did not find any excessive granulation tissue growth during the early stages of wound healing in the Nasopore group, and did not encounter postoperative major bleeding associated with Nasopore. Rather, we found more cases in the Merocel group with discomfort and bleeding associated with the packing and its removal. We propose that there might be greater damage to the nasal mucosa during the removal of non-absorbable packing material, as the pressure of the packing is quite strong. Especially in patients with septal deviation or middle turbinate hypertrophy, the nasal mucosa of the septum can be easily damaged during removal of the packing, and this unwanted damage can increase the risk of adhesion and fibrosis of the nasal ostium after DCR [7,10]. The removal and/or reinsertion of packing material may cause major pain or discomfort to patients, because the nasal cavity becomes much narrower than what it was during surgery, after the disappearance of vaso-constrictive effect of epinephrine.
In addition, Nasopore can separate the mucosal surfaces during the critical early post-surgical days when mucosal swelling is heightened. We believe that the use of Nasopore not only helped in the achievement of excellent early hemostasis, but also made endonasal wound care more comfortable by keeping the mucosal tissue separated, especially in patients with a narrow nasal cavity.
Although it is rare, the extrusion of silicone tubing may occur in the early postoperative period before complete absorption of the Nasopore material. However, we did not observe any case of prolapsed tubing in our cases. At week 1 postoperatively, the position of the silicone tube was confirmed while the external part of the material was partially suctioned.
In the present study, there was a larger portion of patients with preoperative canalicular stenosis in the Nasopore group than in Merocel group, partially due to a non-randomized, retrospective study design, and partially due to the small sample size of the Nasopore group. Further prospective randomized comparative study would be necessary.
In conclusion, although the anatomic and functional success rate of DCR was not affected by the packing material itself, an absorbable packing material such as Nasopore would be very helpful in postoperative hemostasis, endonasal wound care, and in reducing discomfort associated with nasal packing. Considering not only surgical success, but also postoperative pain and discomfort in DCR surgery, is important. Especially in cases with a narrow nasal cavity or in cases where intraoperative bleeding is difficult to control, such as the use of blood thinners or cases of thick maxillary bones, we believe the use of an absorbable packing would help elevate patient satisfaction after surgery.





 XML Download
XML Download