

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Epiretinal membrane (ERM) formation after retinal reattachment surgery is called macular pucker, the occurrence of which frequently causes a decrease in vision and metamorphopsia after retinal detachment (RD) surgery [1-3]. Macular pucker is an overlying preretinal membrane, wrinkling the neurosensory retinal surface. The preretinal membrane develops from the proliferation of cells, including retinal pigment epithelium (RPE), retinal glia, perivascular connective tissue, and/or hyalocytes [4-7].
Preretinal membrane formation on the macular area results in contraction and distortion of the retina, which then result in macular striae, retinal vascular tortuosity, and cystoid macular edema. Vitrectomy to remove a macular pucker is a traditional elective vitreoretinal indication [8] and is generally reported to result in an improvement in vision and/or a decrease of metamorphopsia. The incidence of macular pucker formation between scleral buckling and vitrectomy for primary rhegmatogenous retinal detachment (RRD) has been debated. In a previous study, scleral buckling for repair of RRD resulted in pucker formation in 3% to 8.5% of cases [1,9,10]. Recently, the incidence of macular pucker formation after pars plana vitrectomy (PPV) alone as retinal reattachment surgery has been reported. According to one study, vitrectomy for repair of RD showed a higher incidence (12.8%) of ERM than sclera buckling [11]. On the other hand, another study has reported that scleral bucking following retinal reattachment surgery could more frequently lead to macular pucker than vitrectomy [12]. The primary objective of our study was to investigate the incidence and predisposing factors of macular pucker formation after PPV alone as retinal reattachment surgery. The secondary objective was to evaluate the incidence of secondary vitrectomy for macular pucker and overall visual acuity improvement after membrane peeling.
Materials and Methods
We reviewed charts for 284 consecutive eyes (284 patients) that were followed-up after PPV alone for repair of RRD between January 1, 2009 and December 31, 2010. This study was approved by the institutional review board of the University of Inje. All patients of three surgeons were included if they had a history of only PPV without scleral buckling. Patients with a history of tractional components causing RD (such as proliferative diabetic retinopathy and proliferative vitreoretinopathy), previous RD surgery including scleral buckling, PPV with scleral buckling, and PPV with silicone oil tamponade were excluded.
All surgical procedures were initiated with conjunctival displacement in the inferotemporal, superotemporal, and superonasal quadrants using a pressure plate to hold it firmly to the sclera. A 0.72-mm-wide 23-gauge stiletto blade was then inserted at a 15° to 30° angle through the conjunctiva, sclera, and pars plana 3.0 mm from the limbus. The microcannula was then inserted through the conjunctival incision and into the scleral tunnel using a blunt inserter. An Accurus Vitrectomy System (Alcon Laboratories, Fort Worth, TX, USA) was used for all surgical procedures at a cutting rate of 1,500/min and a suction rate ranging between 150 and 400 mL/min. All patients underwent complete PPV with induction of the posterior vitreous detachment using a triamcinolone acetate stain. The peripheral vitreous was shaved under scleral depression to remove peripheral cortical gel. Subretinal fluid was drained through existing retinal breaks or retinotomies. In cases of bullous peripheral RD, perfluorocarbon liquid (PFCL) was used to flatten the posterior retina. Endolaser photocoagulation was used for retinopexy in the limited areas of retinal breaks, suspected zones, or predisposing lesions. Twenty percent SF6 or 16% C3F8 gas was flushed through the eye after a complete fluid gas exchange was performed. The use of fourth port intraocular chandelier lighting was optional. Patients were instructed to assume the appropriate head position.
The mean follow-up period after RD surgery was 15.2 months and ranged from six to 24 months. To define an ERM, we used clinical biomicroscopy and optical coherence tomography (OCT). ERM peeling was indicated when best-corrected visual acuity was less than 0.5 in decimal units (0.3 or more [logarithm of the minimum angle of resolution, logMAR]) or decreased more than two lines (0.2 or more [logMAR]) after macular pucker diagnosis. Macular pucker was treated using standard three-port 23-gauge PPV and ERM peeling using intraocular forceps.
We reviewed the charts for incidence and predictor factors of ERM formation after PPV alone for repair of primary RRD. In addition, we surveyed for retinal reattachment rates, intraoperative factors, and postoperative complications. We investigated clinical outcomes between the clinically followed macular pucker group and the surgically-treated macular pucker group. Statistical analysis was performed using SPSS ver. 11.0 (SPSS Inc., Chicago, IL, USA). Differences between the groups were calculated using an independent t-test, chi-square tests and Mann-Whitney U-test. Statistical significance was accepted if p < 0.05.
Results
Of 284 patients, 264 completed the six-month follow-up and were the subjects of this analysis, while 20 patients (7.0%) were lost to follow-up. We analyzed a total 264 consecutive eyes (264 patients) which were treated by PPV alone for primary RRD. A description of the patient at the time of enrollment is given in Table 1. Baseline characteristics included age, sex, lens status, characteristics of retinal break (size, number, and location), macular status (on or off), preoperative visual acuity (logMAR), and time lag between symptom presentation and RD repair.
Of these 264 eyes (264 patients), macular pucker was obviously developed on 16 (6.1%) at clinical examination during follow-up. The general profile of macular pucker eyes is shown in Table 2. There were eight (50%) males and eight (50%) females, with an average age of 58.8 years (range, 38 to 79 years). We found a preponderance of elderly patients in the macular pucker group (macular pucker group 58.8 years vs. non-macular pucker group 51.9 years). A slightly lower proportion of eyes with pseudophakia (74 eyes, 28.0%) were found in the study population, and three aphakic eyes were included in the non-macular pucker group. There was a predominance of pseudophakic eyes (five eyes, 31.2%) in the macular pucker group. We did not detect a statistically significant difference in age, sex, or lens status between the macular pucker group and the non-macular pucker group.
In order to analyze the characteristics of retinal break, we defined a large retinal break as greater than two disc diameters. There was a preponderance of multiple (50.0% vs. 27.0%) and large (25.0% vs. 8.9%) retinal breaks as well as a higher percentage of superior retinal breaks (68.8% vs. 65.7%) in the macular pucker group than non-macular pucker group. The statistical analysis of characteristics of retinal breaks between the two groups showed that multiple and large retinal breaks could be predictive factors of macular pucker formation. However, the location of retinal breaks was not an eligible risk factor for macular pucker formation. Through the evaluation of macular status (on or off) of RD, we found no significant difference between the two groups (percentage of macular off RD, 81.3% vs. 73.8%). In the macular pucker group, the time lag between symptoms of RD and surgery for repair of RD was longer than that in the non-macular pucker group (7.42 days vs. 6.34 days). The preoperative visual acuity in the macular pucker group was worse than that in the non-macular pucker group (1.92 logMAR vs. 1.75 logMAR). However, neither factor (time lag or preoperative visual acuity) demonstrated a statistically significant difference between the two groups. The intraoperative and postoperative characteristics of the two groups are shown in Table 3.
During the intraoperative procedure, PFCL was used to flatten the posterior retina in 35 eyes (14.1%) in the non-macular pucker group and three eyes (18.8%) in the macular pucker group. Laser photocoagulation for retinopexy of breaks was used instead of cryopexy. The extent of endolaser photocoagulation for retinopexy was defined by quadrant; the average area was 3.08 quadrants in the macular pucker group and 2.83 quadrants in the non-macular pucker group. Combination surgery with cataract extraction was performed only if sufficient retinal visualization for PPV could not be achieved. This combination surgery was performed on 16 eyes (6.5%) in the non-macular pucker group and in no eyes in the macular pucker group.
Iatrogenic retinal breaks occurred in 25 eyes (10.1%) in the non-macular pucker group and two eyes (12.5%) in the macular pucker group. Retinal breaks were created by vitreous incarceration in the sclerotomy site and traction force on the degenerative retinal areas during peripheral vitrectomy. All iatrogenic retinal breaks were treated with retinopexy by endolaser photocoagulation. These intraoperative factors (PFCL, extent of retinopexy, combined surgery, and iatrogenic retinal break) were not considerable risk factors for macular pucker formation (p > 0.05).
With a single surgery, the detached retina was reattached in 227 eyes (91.5%) in the non-macular pucker group and in 16 eyes (100%) in the macular pucker group. In the non-macular pucker group, 16 eyes (6.5%) needed two additional procedures, and five eyes (2.0%) needed three or more procedures. Ultimately, the detached retina was reattached in all cases in both groups. The causes of primary failure in the non-macular pucker group were a new break in eight eyes (3.2%) and the development of proliferative vitreoretinopathy (PVR) in 13 eyes (5.2%). PVR developed in only one eye (6.3%) in the macular pucker group, and there was no statistically significant difference based on PVR and multiple operations for risk factors of macular pucker formation between the two groups. Postoperatively, vitreous hemorrhage developed in 20 eyes (8.1%) in the non-macular pucker group, whereas four eyes (25.0%) in the macular pucker group developed vitreous hemorrhage. There was a significant difference between the two groups (p < 0.05).
Other postoperative complications such as cystoid macular edema (CME), increased intraocular pressure (IIOP) >21 mmHg that required treatment after two weeks, and development of cataract that required cataract extraction within the six-month follow-up period were investigated. As shown in Table 3, there was no statistically significant difference in CME, IIOP, or cataract between the two groups throughout the follow-up. Infectious complications, such as endophthalmitis related to PPV, were not observed in the follow-up period.
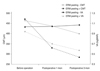
The mean time from primary vitrectomy for RD to diagnosis of ERM was four months. Of 16 eyes with macular pucker formation, ten underwent secondary vitrectomy with ERM peeling for removal of macular pucker (Table 2). In the surgically-treated macular pucker group, the average time interval between confirmation of macular pucker and secondary vitrectomy with ERM peeling was 3.9 months. Consequently, the average period from primary PPV for RD repair to ERM peeling for macular pucker was 7.9 months. The mean vision improvement by ERM peeling surgery was 0.37 (logMAR), and the average central macular thickness (CMT) after ERM peeling surgery was decreased about 187.1 µm (Fig. 1). These results show the correlation between visual acuity and CMT in the macular pucker group (p < 0.05). No other factors were found to be significant between the clinically followed macular pucker group and the surgically-treated macular pucker group.
Discussion
Previous studies have attempted to evaluate the incidence of macular pucker formation after repair of RD. As a result, these studies assessing the preretinal membrane formation after scleral buckling repair of RD estimated the range to be 3.5% to 8% [1,9,10]. However, the incidence of ERMs after repair of RD by PPV alone was estimated to have a varied outcome with a range of 3.6% to 12.8% [11,12].
The primary objective of our study was to assess the incidence (6.1%) of macular pucker formation after PPV alone for repair of RRD. The outcome of our study is similar to that of scleral buckling for repair of RD. In a previously suggested hypothesis, macular pucker formation after the repair of RD was developed by proliferation of cells including RPE, retinal glia, and other progenitor cells. These cells could be dispersed by surgical procedures. In scleral buckling surgery, RPE cells and other progenitor cells are dispersed through the retinal break into the vitreous cavity. In particular, in large retinal breaks greater than three disc diameters, cryoapplication could easily cause the cells to flow out [10]. In pars plana vitrectomy, by vitreous removal and suctioning of subretinal fluid through a peripheral break or a posterior retinotomy, RPE cells and other progenitor cells could be scattered more freely [11]. In our hypothesis, the air-fluid exchange method in PPV could remove most of the dispersed cells, whereas, in scleral buckling surgery, there is no way to eliminate the dispersed cells and reduce additional dispersion. Repair of RD by scleral buckling could cause the dispersed cells to remain in the vitreo-retinal interface in greater numbers than with PPV. The possibility of macular pucker formation could increase if more cells were located in the vitreo-retinal interface. Based on our hypothesis, the difference in the incidence of macular pucker formation after PPV should not be more than but equal to or less than that of scleral buckling (range 3.5% to 8%). The incidence (6.1%) in our study was well correlated with this expectation. As compared with a previous study demonstrating a higher incidence than scleral buckling [11], our study showed that sutureless 23-gauge vitrectomy could reduce production and release of inflammatory factors. Proliferation of the RPE and progenitor cells declined with reduction of the inflammatory reaction. Placement of an intraocular gas for tamponade in a sitting positioning may reduce the concentration of these cells over the macular area compared to that in a face down positioning, decreasing macular pucker formation. Comparing with macular pucker formation after scleral buckling and PPV alone is very difficult work. Previous studies (repair of RD by scleral buckling) were different from our study due to patient populations, follow-up periods after RD repair, and criteria used to define a macular pucker [1,5,10,13,14]. In our study, macular pucker was included when detected by clinical biomicroscopy and confirmed by OCT on follow-up. We excluded other vision-affecting factors (i.e., previous retinal surgeries, proliferative vitreoretinopathy, vitreous hemorrhage, choroidal hemorrhage, degenerative retinal disease, and preoperative macular membranes) except for RD. As a result, we could not exclude the possibility that the incidence of macular pucker formation was underestimated. In previous studies, age [10], cryopexy [10], multiple operations [10,14], proliferative vitreoretinopathy [10,14], macular detachment [14], vitreous hemorrhage [14], low preoperative visual acuity [13], choroidal hemorrhage [13], multiple tear [10], large break, pseudophakia and aphakia [15] were identified as predisposing factors for ERM formation after repair of RD.
In our investigation, we evaluated age, sex, lens status, characteristics of retinal break, macular status, preoperative visual acuity, and time lag before repair of RD as possible predictive factor of macular pucker formation. As a result, age, sex and lens status were not risk factors for macular pucker formation. Unlike other studies, which found macular involvement and retinal break location to be a predictive factor [10,13,14], our investigators detected no significant difference between the two groups. However, multiple and large retinal breaks were possible risk factors for macular pucker formation. Therefore, it seems that size and number of retinal breaks are more important factors than location in terms of dispersion of RPE, retinal glia, and other progenitor cells for macular pucker formation. This is in line with the work of Cox et al. [15], who also found a higher incidence of macular pucker in patients with multiple or large retinal breaks. Although lower preoperative visual acuity and a longer time lag were shown in the macular pucker group, there was no statistically significant difference between the macular pucker group and the non-macular pucker group.
Different from the study of Uemura et al. [10], who reported cryotherapy for retinopexy as a risk factor, intraoperative laser photocoagulation for retinopexy was not a risk factor of ERM formation in our study. Other intraoperative variables such as use of PFCL, combination surgery, and extent of retinopexy were not contributing risk factors for macular pucker.
As shown in Table 3, our finding of retinal reattachment with a single surgery in 243 eyes (92.0%) is similar to a previous study assessing the anatomical success rate of RD surgery [16,17]. Twenty-one reoperations were deemed necessary for RD repair in the non-macular pucker group. Our finding that multiple operations is not a risk factor for membrane formation is in conflict with those of Uemura et al. [10] and Tanenbaum et al. [14].
Vitreous hemorrhage developed more frequently in the macular pucker group than in the non-macular pucker group. This finding is similar to previously reported results of Tanenbaum et al. [14], who posited vitreous hemorrhage as a risk factor of ERM formation. It seems that other progenitor cells dispersed with vitreous hemorrhage could induce preretinal membrane formation. The secondary objective of our study was to evaluate the incidence of secondary vitrectomy for macular pucker and overall visual acuity improvement after membrane peeling. In our study, we found that 3.8% (ten of 264 eyes) of all enrolled patients and 62.5% (ten of 16 eyes) of the macular pucker group underwent secondary vitrectomy with ERM peeling. In this ERM peeling group (surgically-treated macular pucker group), the mean time to ERM peeling surgery was 7.9 months. A secondary operation for macular pucker resulted in an average visual improvement from 0.94 to 0.57 (logMAR). There was no statistically significant difference based on macular involvement or location of retinal tear between the clinically followed macular pucker group and the surgically-treated macular pucker group. The average visual improvement after a secondary vitrectomy with ERM peeling did not show a statistically significant difference between patients with macula-on detachments and patients with macula-off detachments. We observed that the average central macular thickness after membrane peeling declined from 470.7 µm to 283.6 µm. Our finding that the average visual improvement due to macular pucker peeling was directly correlated with the decrease of CMT is consistent with a previous study assessing the role of ERM peeling for idiopathic preretinal membrane [18]. In our study, the use of a retrospective approach is the main limitation, but it is significant that our investigation had twice the number of patients than a previous study (264 eyes vs. 141 eyes) [11].
In summary, we found a 6.1% incidence of macular pucker formation after RD repair by PPV, with two-thirds of the patients undergoing reoperation for membrane peeling. This rate is less than past reports of macular pucker formation after PPV alone. In our study, we found that multiple retinal breaks, large retinal breaks, and postoperative vitreous hemorrhage were associated with a higher rate of macular pucker formation. Therefore, in such cases, clinicians should carefully perform the surgical procedure and conduct a rigorous inspection at every follow-up visit. In addition, we found that macular pucker surgery resulted in a significant increase in vision. However, this study's limitations were a short term follow-up period and its retrospective nature. Thus, this research topic needs to be investigated further in a controlled, prospective trial.



 XML Download
XML Download