

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Intravitreal injections of corticosteroid are recommended for a broad spectrum of ophthalmologic conditions. A beneficial role of intravitreal steroid injections has been reported for diabetic macular edema, exudative age-related macular degeneration, macular edema secondary to retinal vein occlusion, chronic uveitis, and pseudophakic cystoids macular edema [1,2].
Intravitreal steroid injections have potential complications, such as cataract development, increased intraocular pressure (IOP), retinal hemorrhage, retinal detachment, and endophthalmitis [3]. Although steroids reduce local inflammation and retinal edema, they simultaneously decrease local defenses against pathologic agents [3-10]. Viral retinitis following intravitreal triamcinolone acetonide injections (IVTAs) in immunocompetent patients has been reported [3-10], suggesting an association between intravitreal steroids and opportunistic infections. However, the association among intravitreal injection of corticosteroid, viral retinitis, and the pathogenesis of viral retinitis has not been determined. In this report, we present a case of viral retinitis following IVTA in an immunocompetent patient and review the relevant literature.
Case Report
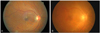
A 56-year-old man presented to our uveitis clinic for evaluation of a visual disturbance in his right eye. He had been diagnosed with diabetes four years previously and was controlling blood glucose with oral medications. His visual acuity was 20 / 40 in the right eye (OD) and 20 / 30 in the left eye. Fundus examination showed moderate non-proliferative diabetic retinopathy in both eyes and macular edema OD (Fig. 1). The foveal thickness was 465 µm OD as observed by optical coherence tomography (OCT; Stratus OCT, Carl Zeiss Meditec, Dublin, CA, USA). We administered IVTA (4 mg) for treatment of the diabetic macular edema using an aseptic technique including irrigation of the conjunctival sac with diluted betadine solution and prescribed oral and topical antibiotics for one week after injection. After IVTA, the visual acuity improved to 20 / 32 OD and the macular edema decreased to 357 µm OD on OCT.
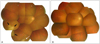
Five months after the IVTA, the patient returned to our clinic for right eye visual deterioration. The visual acuity was 20 / 200 OD and the intraocular pressure was 23 mmHg according to Goldmann applanation tonometer (GAT) measurement. Slit lamp examination of the right eye revealed fine keratic precipitates on the corneal endothelium and moderate (grade +2 inflammatory cells) inflammation in the anterior chamber. Fundus examination showed severe generalized arterial obstruction, vitreous opacity, and a white necrotic retina in the inferotemporal periphery (Figs. 1B and 2A, black arrows). Remnant triamcinolone particles were still visible in the inferior vitreous. (Fig. 2A, white arrow) After presumed diagnosis of viral retinitis, in particular acute retinal necrosis, laboratory work-up, including anterior chamber paracentesis for viral polymerase chain reaction (PCR), was performed. However, no viral DNA was detected by PCR, including herpes simplex virus (HSV), varicella zoster virus (VZV), cytomegalovirus (CMV), or Ebstein-Barr virus. Blood tests for human immunodeficiency virus and syphilis were negative, and the CD4 cell count was within normal limits. Intravenous acyclovir was administered for ten days, and oral valaciclovir was given for the following three weeks. Along with antiviral medications, oral aspirin and oral/topical steroids were prescribed. One week after initiation of antiviral medications, the size of the white retinal necrotic area decreased and eventually disappeared at one month (Fig. 2B). Barrier laser was performed around the necrotic retina for prevention of retinal breaks and detachment. After three months, blood samples for viral serology testing were collected. Anti-HSV, anti-CMV, and anti-VZV IgG were detected, but the IgM titers were negative. During routine six month follow-up visits, the visual acuity was limited to 20 / 100 OD due to cataract and epiretinal membrane (ERM). One year after the IVTA, vitrectomy for ERM removal combined with cataract operation was performed, and the visual acuity was restored to 20 / 40 OD.
Discussion
Our case is presumed to be a form of acute retinal necrosis (ARN) considering the prompt response to antiviral treatment, serum viral IgG results, and typical clinical presentations, although we failed to reveal the causative organism by PCR or serology. The causative association between IVTA and ARN was presumed by the visualization of triamcinolone particles at the time of ARN occurrence and no underlying systemic immune deficiency.
Other possible diagnoses include CMV retinitis and intraocular lymphoma. In CMV retinitis, early lesions are located along the retinal blood vessels and sometimes on the fovea or disc. Intraocular lymphoma/leukemia could also produce whitish infiltrative subretinal lesions. However, in our case, ARN is the more likely diagnosis because a yellow-white retinal lesion was initially noticed in the peripheral retina, and occlusive vasculopathy involving all retinal arteries was observed with anterior chamber reactions, which are the pathognomonic findings of ARN. Follow-up examination showed no evidence of lymphoma or leukemia.
To date, there are 12 case reports of necrotizing herpetic retinopathy, including nine of CMV retinitis and three of ARN in ten immunocompetent patients, of whom two immunocom-promised patients received intravitreal corticosteroid injections (Table 1) [3-11]. The mean age of patients with necrotizing herpetic retinopathy associated with intravitreal corticosteroid injection ranged from 30 to 77 years (range, 63.75 ± 14.13 years). PCR was performed for diagnosis of pathogens in all cases except one [6], which had a lack of vitreous due to previous vitrectomy. The diagnosis was confirmed in seven cases (63.6%) by detection of viral DNA. The IOP of the infected eye according to the available IOP data in case reports was 23 to 48 mmHg (mean, 32.8 ± 10.7 mmHg). Elevated IOP is a common clinical feature of necrotizing herpetic retinopathy associated with intravitreal corticosteroid injection. All case reports mentioned inflammatory cells in the anterior chamber. The interval between intravitreal corticosteroid injection and retinitis ranged from three weeks to seven months (range, 4.0 ± 1.7 months).
Local immune deficiency by intravitreal steroid injections has been suggested as the most likely pathogenesis for necrotizing herpetic retinopathy [3-10]. A history of viral retinitis, such as CMV retinitis, was not clear except in only one case of CMV retinitis. However, reactivation of a virus from prior subclinical infections may play an important role in viral retinitis after IVTA, as well as in new viral infections.
Bacterial endophthalmitis, one of the most serious complications of an IVTA, presents 7.5 days after injection [12], which is earlier than that of necrotizing herpetic retinopathy (four months on average). Bacterial endophthalmitis usually develops through the inoculation of bacteria into the sterile vitreous, whereas necrotizing herpetic retinopathy can develop by reactivation or by new inoculations. Beer et al. [13] reported that triamcinolone was detected in the aqueous humor more than three months after IVTA. Moreover, triamcinolone can remain in the vitreous longer than in the aqueous humor [14]. The persistent immunocompromised state of the posterior segment after IVTA appears to mimic the intraocular state of the immunocompromised patient and may be the main mechanism of viral retinitis, either by reactivation or by a new infection of a virus.
In conclusion, we report a case of presumed ARN after IVTA and propose that physicians should be aware of the possibility of necrotizing herpetic retinopathy after IVTA. Heightened suspicion and prompt treatment using antiviral agents could act to preserve visual acuity.

 XML Download
XML Download