

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Since tissue glue was first reported in the management of corneal perforations in 1968 by Refojo et al. [1] and Webster et al. [2], it has been widely used in ophthalmology. Several case series have reported the successful use of tissue glues in various corneal and conjunctival surgeries, as well as corneal perforations [3-18]. Cyanoacrylate-based glue, fibrin-based glue, and other new synthetic agents are currently available. However, these glues were used cautiously in septic conditions because the corneal lesions might have been concealed by the opaqueness of the glue and resistant organisms could have developed. We report a case of bacterial keratitis, which was aggravated and superimposed by a fungal infection after the application of fibrin glue to manage an impending perforation. This is first case of a mixed infection after gluing.
Case Report
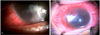
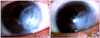
A healthy 27-year-old woman was referred to our hospital for a nonresponsive, progressive corneal ulcer in the left eye. One month before visiting our clinic, she went to a local ophthalmic clinic complaining of irritation, redness, and pain in the left eye, where a corneal ulcer was diagnosed and topical gatifloxacin and tobramycin were given alternatively every hour. Her symptoms still persisted and infection became aggressive, despite eyedrop application. The medication was increased to an hourly fortified topical cefazolin at a dosage of 50 mg/mL. One week after eyedrop application, fibrin gluing with bandage contact lens was done twice, due to the impending perforation of the thinned ulcerative area. The initial culture revealed no growth. The patient was then referred to our department for further evaluation. On examination, the best-corrected visual acuity was 20 / 20 in the right eye and hand movement in the left eye. She had an uncertain history of keratitis in her left eye several years prior. A slit lamp examination of her right eye was unremarkable. The left eye showed a large ulcer, measuring 5 × 3 mm, with an overlying fibrin gluing patch (Fig. 1A). A lesion was located at the inferotemporal cornea, adjacent to the limbal area. Severe chemosis and lid swelling were combined, but intraocular or orbital dissemination was not found on a B-scan ultrasound and an orbit computed tomography exam. The anterior chamber was maintained without chamber collapse and observed as an inflammation of 2+ cells without a hypopyon. Feathery-like infiltration was observed at the margin of the lesion, even when obscured by overlying fibrin glue. Topical amphotericin B (0.15%) was applied every hour. Corneal scraping was not performed and disease progression was observed for two days, because the lesion margin was overlaid with the gluing patch and the risk of perforation was high when the glu ing patch was handled. The ulcer lesion slowly progressed and the symptoms, including ocular pain, conjunctival injection was aggravated. We decided to remove the gluing patch and perform a corneal scraping and biopsy with a multiple amniotic membrane graft to seal the thinned or perforated cornea. When the overlying fibrin glue was carefully removed, a masked lesion was revealed. Necrotic, infiltrated debris had expanded, surrounding the lesion, and an iridocorneal adhesion under the ulcerative lesion was observed (Fig. 1B). Micro-leaking was found at the center of the thinned ulcer base. Corneal scraping for microbiologic evaluation was carefully done at the ulcerative base and margin and necrotic tissue was also debrided to improve drug penetration. The adhesiolysis was done between the iris and cornea. A three-layered amniotic membrane was patched over the ulcerative lesion and the outermost layer covered the lesion over 3 mm from the margin of the lesion, including the half cornea and limbus. Finally, intracameral cefuroxime (1 mg/0.1 mL) and amphotericin B (0.5 µg/0.1 mL) were injected. On the second day after the surgery, the size of the ulcer had decreased and the conjunctival injection, lid swelling, ocular pain gradually improved. Three days after the surgery, the corneal cultures grew Fusarium, as well as Enterococcus faecalis. Fortunately, Enterococcus faecalis is susceptible to levofloxacin and cephalosporin. Topical amphotericin B (0.15%) and gatifloxacin were still continuously administered hourly and the patient was also started on oral itraconazole. Topical cycloplegics and antiglaucomatics were added to control the pain and lowering the intraocular pressure, respectively. Topical amphotericin B and gatifloxacin were reduced to four applications per day after one week. Three weeks after surgery, the outermost layer of amniotic membranes, as the temporary patch, was removed. The anterior chamber was observed to be clear without cells (Fig. 2A). All antifungal medications were discontinued, as the infection sign was clinically and symptomatically clear four weeks later. Two months after surgery, the lesion was totally opaque and sclerotic and the thinned area was enhanced by permanent multiple amniotic grafts and the overlying epithelium was well maintained (Fig. 2B). A best-corrected visual acuity was recovered to 20 / 60 in the left eye.
Discussion
Corneal thinning or perforations can result from a variety of ocular disease states associated with trauma, acute or chronic inflammation. Regardless of the cause, perforation creates an emergent situation and prompt treatment is necessary. Many surgical approaches, such as tissue adhesive, bandage contact lens, conjunctival flap, and therapeutic penetrating keratoplasty, have been introduced to treat perforated ulcers of the cornea. Corneal transplant is a definitive treatment, but preserved cornea are of limited supply, and preceding temporary patching with the management of the underlying disease is emphasized.
Tissue glues have been used in ophthalmology to treat corneal thinning and perforations, and ocular surface disorders. Several case series have reported the successful use of fibrin glues, as well as cyanoacrylate glues, in the management of corneal perforations. According to a report by Sharma et al. [19], even though the properties of cyanoacrylate and fibrin glue seem very different, their success in sealing corneal perforations appears to be similar. In the management of 41 corneal perforations, they found that both fibrin and cyanoacrylate glues were similarly very effective in the closure of corneal perforations up to 2 mm in diameter.
However, the use of tissue glue in treating infectious ulcerations has been limited in practice. The development of infectious infiltrates after prolonged cyanoacrylate glue adhesion has been documented in numerous studies [14,17]. The symptoms and signs of the infectious ulcers may have been concealed by the opaqueness of the glue. Furthermore, the development of resistant organisms should be considered. For this reason, the use of antibiotic prophylaxis is recommended while the cyanoacrylate glue is applied and the antibiotic may be changed periodically to minimize the growth of resistant organisms [9]. Also, the efficacy of antibiotics in treating infectious ulcerations may be limited due to tissue necrosis or overlying glue itself.
In this case, a fibrin glue without a covering layer was used to manage the impending perforation in infectious keratitis. To our knowledge, this case is the initial report in which a secondary infection developed after the use of fibrin glue, although several cases of corneal ulcers by mixed microorganisms were previously reported in Korea [20,21]. Despite the same medications, the keratitis was improved only by the removal of the overlying fibrin glue. We considered three aggravating factors in this case. Firstly, necrotic tissue and bandage contact lenses may interrupt the antibiotics delivery, promoting microbiologic colonization. Secondly, low-inflammatory properties of fibrin glue may prove disadvantageous in circumstances where vascularization is desired, such as infectious ulcers. This is similar to the principle of conjunctival flaps in the management of refractory corneal ulcers. Finally, it is assumed that the application of fibrin glue in perforated infectious ulcers has the same limitations as cyanoacrylate glue. In contrast to the cyanoacrylate glues as synthetic adhesives, the benefits of fibrin glue relates to its biodegradability and flexibility. The bonding that occurs with fibrin glues simulate the final stage of the coagulation cascade, producing a biocompatible fibrin matrix similar to a natural plasma clot. Although the fibrin glues have a lower tensile strength and slower polymerization, they may induce minimal inflammation, due to their being biologic and biodegradable [22]. Although there is no comparative study of the drug penetration between the cyanoacrylate and fibrin glues, it is expected that fibrin glues, which are more biocompatible than cyanoacrylate glues, may be advantageous in their management of infectious corneal perforation. In experimental studies, fibrin glue has also been used as a vehicle for delivering antibiotics and platelet gel, potentially containing natural healing factors that promote tissue regeneration [23-26]. However we found in this case that the application of fibrin glue to a perforated infectious ulcer aggravated the ulcer lesion and caused a secondary infection to deveop.
In conclusion, fibrin glue is useful in the treatment of corneal perforations and corneal thinning, but it has also the risk of microbial colonization, and secondary infection, as with cyanoacrylate glue. The use of fibrin glue should be avoided, especially in infectious keratitis, and prophylactic antibiotics should be used even in sterile keratitis, because lesion can be aggravated and a secondary infections may develop. Future studies may reveal pharmacologic properties or biochemical effects on tissue for each of the available glues, and newer compounds may be developed with better biocompatibility or drug penetration.
 XML Download
XML Download