

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Sulfa-derivative drugs, such as topiramate [1], sulfamethoxazole, sulfasalazine, indapamide, and acetazolamide have been reported to cause acute bilateral myopia and angle closure [2-3]. Hydrochlorothiazide (HCTZ) is a first-line diuretic drug of the thiazide class that acts by lowering peripheral vascular resistance and inhibiting the ability of the kidneys to retain water [4]. HCTZ is a sulfa derivative and has been reported to provoke acute myopic shift and bilateral acute angle closure glaucoma [5]. We are unaware of any previous reports of HCTZ-induced acute myopic shift and intraocular pressure (IOP) elevation in Korea. Here, we relate the cases of two patients who presented with acute-onset bilateral myopia and ciliochoroidal effusion secondary to HCTZ and describe the clinical features of HCTZ-induced myopia.
Case Reports
Case 1
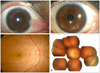
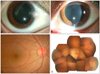
A 45-year-old woman presented with acute bilateral visual deterioration with duration of one day. Her visual acuities had previously been good without corrective lenses. She had been taking fluoxetine, magnesium hydroxide, and HCTZ for one month to reduce her weight. She had visited another local ophthalmic clinic on the day of symptom onset, and had been told that the IOPs of the right and left eyes were 37 and 41 mmHg, respectively. She was prescribed topical IOP-lowering drugs, namely, Cosopt® (dorzolamide hydrochloride-timolol maleate) and Xalatan® (latanoprost), and oral Diamox® (acetazolamide). Her uncorrected visual acuities (UCVAs) were 0.15 (20 / 150), oculus dexter (OD) and 0.1 (20 / 200), oculus sinister (OS). Automated refraction revealed bilateral myopia with spherical equivalents of -3.0 diopters (D), OD and -3.6 D, OS. Degree of myopia was unchanged by cycloplegic refraction (Table 1). After correcting measured refractive errors, she could see 1.0 (20 / 20) with either eye. Her IOPs were 12 mmHg, OD and 14 mmHg OS by Goldmann applanation tonometry. An anterior segment examination revealed conjunctival chemosis and injection, shallow anterior chambers, and narrow angles in both eyes (Fig. 1A and 1B), and a funduscopic examination revealed bilateral choroidal effusions in the 360o periphery (Fig. 1D) and radiating retinal folds in the macula (Fig. 1C). She was diagnosed as having drug-induced myopia and asked to discontinue drugs including HCTZ. Ten days later, she reported that her vision had recovered and that all ocular changes had disappeared (Fig. 2). At this time, her UCVAs were 0.8 (20 / 25), OD and 0.6 (20 / 33), OS and she had a best-corrected visual acuity (BCVA) of 1.0 (20 / 20) in both eyes. Myopia had been reduced to the prior refractive state (spherical equivalent of -0.75D, oculi unitas).
Case 2
A 40-year-old woman presented with bilateral visual acuity deterioration, which had started 9 hours before presentation. She also had good visual acuities without corrective lenses before the episode. She had been prescribed ginexin, spironolactone, and HCTZ at the local clinic of internal medicine to cure edematous changes of the lower extremities. Her UCVAs were 0.08 (20 / 250), OD and 0.06 (20 / 300), OS. Automated refraction revealed bilateral myopia with spherical equivalents of -4.5 D, OD and -5.25 D, OS and degree of myopia was unchanged by cycloplegic refraction (Table 1). After correcting measured refractive errors, she could see 1.2 (20 / 16), OD and 1.0 (20 / 20), OS. Her IOPs were 15 mmHg, OD and 16 mmHg, OS by Goldmann applanation tonometry. Anterior segment examinations revealed conjunctival chemosis, shallow anterior chambers, and narrow angles in both eyes. She was also diagnosed as having drug-induced myopia and recommended to discontinue all three drugs. Nine days after the discontinuance of medications, her UCVAs were 0.8 (20 / 25), OD and 0.6 (20 / 30), OS and myopia had been reduced to the prior refractive state (spherical equivalent of -0.75 D, OD and -1.25 D, OS). An anterior segment examination revealed that the conjunctival chemosis had disappeared and that the anterior chambers were of normal depth.
Discussion
Both of our patients showed 2 to 4 diopters of transient myopia after HCTZ intake (Table 1). Because HCTZ was the only drug taken by both patients and all ocular signs and symptoms disappeared after cessation of this drug, we concluded that HCTZ was responsible for the acute ocular signs and symptoms. Many reports [1-3,6-10] have been issued on the clinical characteristics of sulfa drug-induced acute ocular changes. In this report, we show photographs of choroidal effusion, radiating retinal folds, and conjunctival chemosis, which have not been previously presented.
The mechanism of acute myopic shift has been suggested to involve ciliochoroidal effusion and an anterior rotation of the ciliary body. Myopic shift occurs due to the anterior migration of the iris-lens diaphragm, which increases focal length. The resulting configuration has a significantly shallower anterior chamber and appositionally closes the angle of both eyes, which precipitates a glaucomatous crisis [2]. The pathophysiology of ciliochoroidal effusion is considered to be driven by an idiosyncratic reaction, and some researchers have suggested that prostaglandins are involved [7,11].
The differential diagnoses should include ciliary muscle spasm and primary angle closure glaucoma. Ciliary muscle spasm occurs as a manifestation of iridocyclitis, but it may also be induced by some drugs like anticholinesterase. The diagnosis of the patient can be confirmed by cycloplegic refraction [12]. In our case studies, refractive errors, as determined by cycloplegic refraction, were similar to those detected by manifest refraction, which allowed us to rule out a ciliary muscle spasm. Furthermore, because primary angle-closure glaucoma seldom develops bilaterally, the differential diagnosis is relatively easy. Other clinical manifestations, such as choroidal effusion, retinal folds, and conjunctival chemosis can also aid in establishing the differential diagnosis.
Treatment of drug-induced myopia requires the prompt withdrawal of the offending agent, though discontinuation of medication should be conducted in consultation with an internist to reduce the likelihood of systemic side effects [6]. A previous report also noted that laser iridotomy is not helpful, since the event is not due to a pupillary block [9].
Whenever a case of bilateral acute myopic shift with shallow anterior chambers and IOP elevation is encountered, drug-induced myopia from ciliochoroidal effusion should be suspected and treated properly.

 XML Download
XML Download