

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To identify predictive factors for recovery time in patients with orbital fracture with diplopia through analysis of preoperative and postoperative computed tomography (CT) images and postoperative recovery time.
Methods
We retrospectively analyzed CT findings-preoperative: fracture size, type of fracture, fracture site, extraocular muscle (EOM) swelling, EOM and soft tissue injury, and the amount of soft tissue herniation; post-operative: degree of enophthalmos, and diplopia recovery period in 379 patients who underwent surgical treatment for orbital fracture between March 2006 and December 2015.
Results
The average postoperative follow-up period was 556.2 ± 59.5 days, and the mean duration of recovery was 23.9 ± 42.5 (range, 3–186) days. The recovery time of diplopia was significantly increased with the following preoperative CT findings: fracture size (small and medium < large) (p = 0.049), type of fracture (linear < hinge < comminuted, trap-door) (p < 0.01), fracture site (inferior < medial and both) (p < 0.01), EOM and soft tissue injury (prolapse and torsion, muscle entrapment, kinked muscle) (p < 0.01), and the amount of soft tissue herniation (small and medium < large) (p < 0.001). The mechanism of injury, sex, age, and the degree of enophthalmos were not related to the length of the diplopia recovery period.
Figures and Tables
Figure 1
The size and type of blowout fracture. The size of the orbital wall fracture classified into small (< 20%) (A), medium (B) and large (> 50%) (C). The type of the orbital wall fracture classified into linear (D), hinged (E), comminuted (F) and trapdoor (G).

Figure 2
Extraocular muscle swelling. The measurement of extraocular muscles (white arrow, short axis; black arrow, long axis).

Figure 3
Soft tissue herniation. Amount of soft tissue herniation classified into small (only soft tissue, small amount) (A), medium (only soft tissue, large amount) (B) and large (soft tissue with muscle, large amount) (C).

Figure 4
Extraocular muscle and soft tissue injury. Extraocular muscle and soft tissue injury type classified into muscle prolapse without torsion (A), muscle torsion without prolapse (B), muscle prolapse with torsion (C), kinked muscle by bone (D), muscle entrapment (E) and soft tissue entrapment (F).

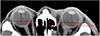


Table 3
The relationship between diplopic period and pre-operative CT features of EOM and soft tissue



References
1. Paek SH, Kim YS, Lee TS. A clinical study of blowout fracture. J Korean Ophthalmol Soc. 1993; 34:1194–1198.
2. Hoşal BM, Beatty RL. Diplopia and enophthalmos after surgical repair of blowout fracture. Orbit. 2002; 21:27–33.
3. Putterman AM, Stevens T, Urist MJ. Nonsurgical management of blow-out fractures of the orbital floor. Am J Ophthalmol. 1974; 77:232–239.
4. Gilbard SM, Mafee MF, Lagouros PA, Langer BG. Orbital blowout fractures. The prognostic significance of computed tomography. Ophthalmology. 1985; 92:1523–1528.
5. Kim HW, Kim YI, Won IK. Clinical analysis of blow-out fracture with ocualr motion limitation: comparison of surgical and conservative treatment. J Korean Ophthalmol Soc. 1999; 40:632–638.
6. Kim SK, Chang HK. The clinical study of treatment of blowout fracture. J Korean Ophthalmol Soc. 1995; 36:1629–1635.
7. Kroll M, Wolper J. Orbital blowout fractures. Am J Ophthalmol. 1967; 64:1169–1172.
8. Lee SY, Kim SY, Kim HB. Orbital fractures evaluated by computed tomography. J Korean Ophthalmol Soc. 1990; 31:249–253.
9. Ahn SK, Jung SW. The clinical aspects of orbital fractures proven by computed tomography. J Korean Ophthalmol Soc. 1997; 38:2077–2083.
10. Hawes MJ, Dortzbach RK. Surgery on orbital floor fractures. Influence of time of repair and fracture size. Ophthalmology. 1983; 90:1066–1070.
11. Hwang K, Huan F, Hwang PJ. Diplopia and enophthalmos in blowout fractures. J Craniofac Surg. 2012; 23:1077–1082.
12. Jin HR, Lee HS, Yeon JY, Suh MW. Residual diplopia after repair of pure orbital blowout fracture: the importance of extraocular muscle injury. Am J Rhinol. 2007; 21:276–280.
13. Lyon DB, Newman SA. Evidence of direct damage to extraocular muscles as a cause of diplopia following orbital trauma. Ophthalmic Plast Reconstr Surg. 1989; 5:81–91.
14. Jung H, Byun JY, Kim HJ, et al. Prognostic CT findings of diplopia after surgical repair of pure orbital blowout fracture. J Craniomaxillofac Surg. 2016; 44:1479–1484.
15. Su Y, Shen Q, Lin M, Fan X. Predictive factors for residual diplopia after surgical repair in pediatric patients with orbital blowout fracture. J Craniomaxillofac Surg. 2016; 44:1463–1468.
16. Kang HJ, Ha MS. A clinical feature of the patients of orbital wall fracture with diplopia. J Korean Ophthalmol Soc. 2009; 50:969–975.
17. Kim HE, Lew H, Yun YS. The size of extraocular muscles estimated by computed tomography in patients undergoing orbital wall fracture repair. J Korean Ophthalmol Soc. 2009; 50:1447–1454.
18. Whitehouse RW, Batterbury M, Jackson A, Noble JL. Prediction of enophthalmos by computed tomography after ‘blow out’ orbital fracture. Br J Ophthalmol. 1994; 78:618–620.
19. Rhee JS, Kilde J, Yoganadan N, Pintar F. Orbital blowout fractures: experimental evidence for the pure hydraulic theory. Arch Facial Plast Surg. 2002; 4:98–101.
20. Ahmad F, Kirkpatrick NA, Lyne J, et al. Buckling and hydraulic mechanisms in orbital blowout fractures: fact or fiction? J Craniofac Surg. 2006; 17:438–441.
21. Emery JM, Von Noorden GK, Schlernitzauer DA. Management of orbital floor fractures. Am J Ophthalmol. 1972; 74:299–306.
22. Greenwald HS Jr, Keeney AH, Shannon GM. A review of 128 patients with orbital fractures. Am J Ophthalmol. 1974; 78:655–664.
23. Cope MR, Moos KF, Speculand B. Does diplopia persist after blow-out fractures of the orbital floor in children? Br J Oral Maxillofac Surg. 1999; 37:46–51.
24. Harris GJ, Garcia GH, Logani SC, Murphy ML. Correlation of preoperative computed tomography and postoperative ocular motility in orbital blowout fractures. Ophthal Plast Reconstr Surg. 2000; 16:179–187.
25. Gosau M, Schöneich M, Draenert FG, et al. Retrospective analysis of orbital floor fractures--complications, outcome, and review of literature. Clin Oral Investig. 2011; 15:305–313.
26. Matsunaga K, Asamura S, Morotomi T, et al. Association between preoperative inferior rectus muscle swelling and outcomes in orbital blowout fracture. J Craniomaxillofac Surg. 2011; 39:509–514.
27. Burres SA, Cohn AM, Mathog RH. Repair of orbital blowout fractures with Marlex mesh and Gelfilm. Laryngoscope. 1981; 91:1881–1886.
28. Converse JM, Smith B, Obear MF, Wood-Smith D. Orbital blowout fractures: a ten-year survey. Plast Reconstr Surg. 1967; 39:20–36.
29. Hartstein ME, Roper-Hall G. Update on orbital floor fractures: indications and timing for repair. Facial plast Surg. 2000; 16:95–106.

30. Shin KH, Baek SH, Chi M. Comparison of the outcomes of non-trapdoor-type blowout fracture repair according to the time of surgery. J Craniofac Surg. 2011; 22:1426–1429.
31. Wilkins RB, Havins WE. Current treatment of blow-out fractures. Ophthalmology. 1982; 89:464–466.
32. Emery JM, Noorden GK, Sclernitzauer DA. Orbital floor fractures: long-term follow-up of cases with and without surgical repair. Trans Am Acad Ophthalmol Otolaryngol. 1971; 75:802–812.
 XML Download
XML Download