

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Individuals with special needs are those who need help for medical and mental or psychological disabilities, and are said to have disability, mental retardation, developmental deficit, or handicap [1]. For such patients, medical treatment should be personalized and the most appropriate medical treatment should be provided [2]. Patients with special health care needs (PSHCN) are more likely to develop health problems, including dental issues [3], and could belong to any race or social class. According to the World Health Organization data, it affects about 3% of the world's population each year, and they constitute 3% of the population of our country. This rate can increase later up to 8.5% due to acquired chronic diseases [45].
A good level of communication with the patient is essential during dental treatments to conduct the procedures smoothly [6]. Because of anatomic deformations or pathophysiological or psychological reasons, these patients may not cooperate at the desired level and dentists cannot provide effective treatment [7]. In some disabled individuals, dental treatment cannot be performed without sedation or general anesthesia. Thus, sedation and general anesthesia are extremely humanistic approaches in these patient groups [89]. Although dental treatments do not pose a risk to the patients' lives, general anesthesia and sedation have serious risks, especially in patients presenting a high score according to the American Society of Anesthesiologists (ASA) classification of physical status, and those with cardiovascular problems and respiratory or central nervous system pathologies. To avoid these risks as much as possible, a thorough preoperative preparation process and optimum conditions for treatment should be followed. The healthcare team serving the patient should have sufficient experience to intervene in a timely, fast, and accurate manner when needed. Patients should not only be under supervision of anesthesiologists and dentists, but also have consultant physicians present who are experts in their respective branches, in order to minimize risk [10]. Although there is sufficient literature on dental treatment modalities used in these patient groups, there are not enough clinical studies on anesthesia use. The majority of anesthesia studies are review articles. In PSHCN, there is no standard anesthetic approach due to varying clinical conditions [11]. Therefore, health practitioners do not have enough experience to deal with this complex patient group. In this study involving a very large database, we aimed to contribute to the literature by sharing our results and experiences about anesthesia applications in PSHCN.
MATERIAL AND METHODS
1. Ethical approval
The Ethics Committee of the Süleyman Demirel University Medical Faculty approved this study(04.07.2018/136).
2. Study population
This study examined records of patients who underwent dental treatment under sedation and general anesthesia, between April 2014 and October 2018, at the Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Süleyman Demirel University.
3. Study design
The dental treatment data related to the PSHCN were obtained from the patient information system. Patients without necessary information or informed consent were excluded from the study. A total of 1045 general anesthesia or sedation procedures were recorded in 710 patient files, including repeated procedures at different times. Demographic data, ASA classification, Mallampati score, anesthesia duration, type of anesthesia, anesthetic and analgesic agents used, dental treatment applied, secondary diseases, and complications seen in the peroperative period were recorded.
4. Patient with special health needs
The PSHN were evaluated under five groups:
Other syndromes (Group II)
This group included patients with syndromes other than Down syndrome (Wilson Syndrome, Costello Syndrome, Russel Silver Syndrome, TORCH Syndrome, Cotard Syndrome, Di George Syndrome, Gilbert Syndrome, Peutz Jechers Syndrome, Williams Syndrome, Orofacial Digital Syndrome, Angelman Syndrome, Asperger Syndrome, Moebius Syndrome, Apert Syndrome, Syndrome, Lesch Nyhan Syndrome, Cohen Syndrome, Sturge Weber Syndrome, Klinefelter Syndrome, West Syndrome, Won Der Knaap Syndrome, Gapo Syndrome, Schwachman Diamond Syndrome, Sweet Syndrome, and Phenylketonuria Syndrome).
Psychiatric disorder (Group III)
This group included patients with autism, bipolar disorder, attention deficit disorder, or schizophrenia.
Physical disabilities (Group IV)
This group included patients with visual impairment, and hearing and speech disability.
Complicated medical story (Group V)
This group included patients presenting mental and/or motor retardation with unclear etiology, cerebral palsy, spina bifida, and hydrocephalus, as well as patients with major deficits originating from the central nervous system and oncology and non-syndromic patients. Patients with several medical problems and undergoing serious medical treatment for the same were also included in this group.
5. Dental treatments
Dental treatments were classified into two groups
simple dental treatments and maxillofacial procedures. The former group included dental examination, teeth extraction, filling, canal treatment, dental ımplantation, and prosthetic procedures under anesthesia, while the latter included surgical treatment of jaw fractures, dental implants, surgical excision of cysts in the jaw, surgical implantation of the maxillary expansion, plaque placement, and disassembly operations.
Preoperative evaluation
Patients who did not cooperate for dental examination and treatment were evaluated preoperatively and physically examined. Laboratory tests and consultations were requested if necessary. Other accompanying pathologies and drugs consumed were noted and necessary precautions were taken. All patients undergoing sedation or general anesthesia were operated after a fasting period of at least 6 h. After explaining about anesthesia and the possible risks, written informed consent was obtained from the legal guardians of these patients.
Intraoperative period
Peripheral oxygen saturation, heart rate, and blood pressure were monitored according to the ASA guidelines during the dental procedures. Different anesthetic agents and methods were used according to the patients' medical and compliance status. After initiation of sedation or general anesthesia in all patients, proper local anesthesia was achieved using ultra-gain (Sanofi/Turkey) before starting dental treatment. Duration of anesthesia in patients was calculated as the time from induction onset to extubation for general anesthesia.
Postoperative period
Postoperatively, the patients were monitored in the recovery unit for 15–30 min. Patients with satisfactory vital functions were put into service. Oral nutrition was started after 1 h of observation in patients sedated with inhalation agent, after 2 h in those sedated with intravenous agent, and after 4 h in those under general anesthesia. The patients who could tolerate the oral intake were discharged on the same day, while those with nausea and vomiting or requirinig more recovery time were followed-up and treated in the in-patient service for 24 h.
6. Statistical analysis
Statistical Package for Social Sciences (version 18.0, Chicago, IL, USA) was used for statistical analysis. Categorical variables were represented as number and percentage, and numerical variables as mean and standard deviation. Chi-square and Fisher's exact test were used for categorical variables. The comparisons of the averages of more than two independent groups of the numerical variables were performed using the one-way analysis of variance test. Post-hoc least significant difference test was used, and P-values <0.05 were considered significant.
RESULTS
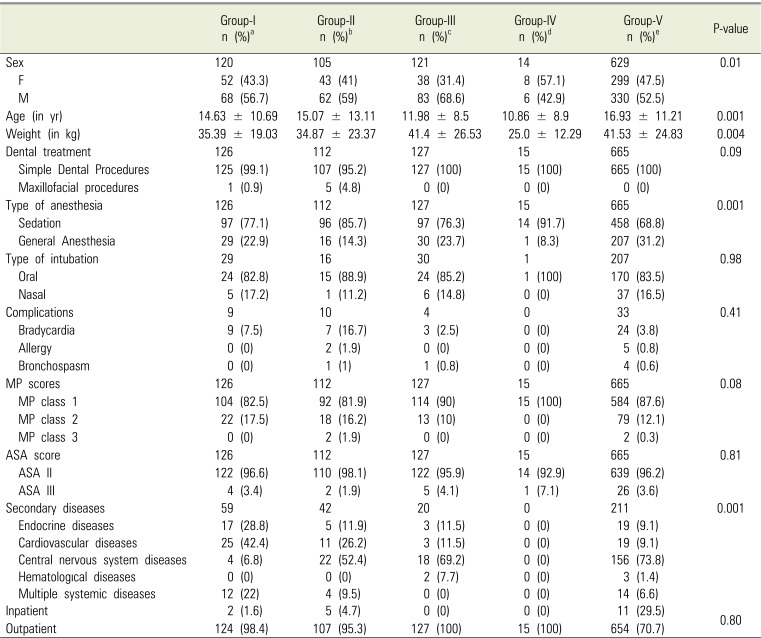
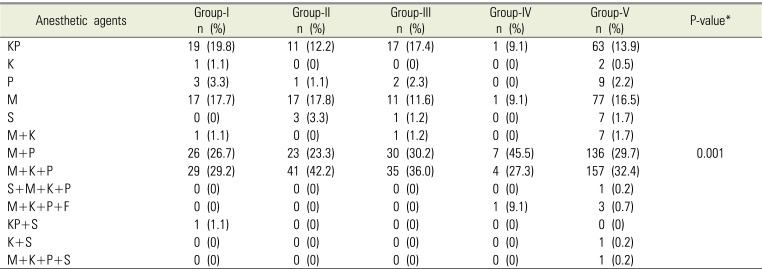
Among 1045 cases in 710 patients (47.5% females, 52.5% males; mean age 15.76 ± 11.17 years, range: 1–68 years), general anesthesia and sedation were performed in 72.9% and 22.1% patients, respectively. The application and clinical findings are summarized in Table 1. The proportion of males was higher in all groups, except in Group IV (57.1% females), and male proportion (68.6%) was more than twice that of females in Group III. These data were statistically significant (P < 0.01). The mean age was the lowest in Group IV (10.86 ± 11.17 years, range: 4–38) and highest in Group V (16.93 ± 11.17 years, range: 1–68), which was statistically significant (P = 0.04). The mean duration of anesthesia was 43.20 ± 35.85 min (range: 3–210). It was second the shortest in Group II (34.29 ± 25.94 min, range: 10–180) and longest in Group V (46.32 ± 38.02 min, range: 3–210), and was statistically significant (P = 0.001). The drugs used in sedation are summarized in Table 2. Pental sodium (İ.E.Ulagay/Turkey) and propofol (Fresenius Kabi/Turkey) were used in 77.4% and 22.6% cases undergoing intravenous induction of general anesthesia, respectively. While local anesthesia was sufficient for analgesia in 90.7% of patients, acetaminophen and tramadol with 3% narcotic analgesic was used in addition to local anesthesia in 7% patients.
DISCUSSION
PSHCN are unable to mainatain adequate oral care and hygiene, as they cannot perform self-care or remove dental plaque from the mouth. Furthermore, problems may intensify due to malocclusion [12], and they present higher prevalence of dental caries as compared to their peers. Especially in this group of patients, sweets given as reward in behavior-change programs can negatively affect their oral health, similar to diet containing dry-fruits leading to constipation [413]. Moreover, they require frequent dental treatment, and most times, their treatment cannot be performed only with local anesthesia [4]. General anesthesia and sedation are an essential part of repetitive dental procedures in such patients [14]. However, these patients are not a homogenous group, and there are varying clinical conditions presented.
There are a limited number of clinical studies in the literature [15]. Due to the complexity of the subject, mental retardation, other syndromes, psychiatric disorders, physical disorders, and complex medical history were compared with healthy patients or with each other [16]. Previous studies have made comparisons of two or three groups [1516], but there are no studies comparing all five groups. Down syndrome is the most frequently encountered syndrome in clinics. There are many case reports and reviews in the literature about anesthesia management and problems related to anesthesia [1718]. In some syndromes, there are several physical defects besides systemic anomalies [1718192021222324]. The clinician would be more comfortable performing the treatment if the patient is immobile during the procedure in order to reach the area of treatment easily. This can only happen under general anesthesia or sedation. Our study was based on the need for anesthesia in such patients. The groups were distributed as homogeneously as possible with respect to their clinical findings. Although this is a complex subject, the common point was that all these patients required special care during dental procedures.
In our study, patients were examined and distributed into five main groups to obtain data and decide the appropriate anesthetic approach.
Group I: Down syndrome usually makes patients hypotonic. These patients show joints with flask-like structure, large tongue, short neck, and limited atlanto-occipital joint movement (5%). Major cardiac anomalies (atrioventricular septal defect, patent ductus arteriosus) may be seen in 40% of Down syndrome patients [17]. In our study, cardiovascular diseases were observed in 42% patients of this group. These patients received antibiotic prophylaxis before dental treatment. They may also present respiratory system-related anomalies such as subglottic stenosis, abnormally large tonsils and adenoids, and obstructive sleep apnea syndrome. Usually, epilepsy is observed in 5–10% of the patients and hypothyroidism in 50%; however, in our group of patients, 6.8% presented epilepsy and 28.8% presented endocrine diseases. These patients also show duodenal atresia, gastroesophageal reflux, and are at 12 times more risk of pneumonia and obesity. All this leads to difficulty in airway and vascular access. Mallampati class 2 score was most prevalent in this group. Diseases affecting the cardiac, respiratory, and central nervous system increases risk of morbidity. These patients also have atropine sensitivity [18]. In our study, Down syndrome patients presented severe bradycardia, which was unlike the other groups. We preferred sedation because of intubation difficulty. In sedation, we avoided breathing and depressing doses, and the combination of ketofol was most used in this group.
In Group II comprising of syndromes other than Down syndrome, patients had abnormal teeth and jaws. Due to lip-biting habit, facial deformities were noticed, which were subsequently caused by self-injurious practices. Therefore, maxillofacial procedures were performed in this group. The literature on these syndromic patients consisted of case reports or rewiews [192021222324]. Due to the rare occurrence of these syndromic cases, some cases had never been encountered before professionally. The presence of life-threatening anomalies in these patients indicated shortening the anesthesia duration as much as possible. Group II showed the second shortest period of anesthesia, and procedures were divided. Using one agent for sedation was more prevalent in this group. We believed that establishing appropriate anesthetic conditions with the least possible medication in these patients would reduce the anesthetic complications. Optimal treatment could not be performed in these patients, and only symptomatic treatment was performed instead of restorative treatment. Tooth extraction was performed using sevoflurane inhalation because of the difficulty in vascular access. The average duration of anesthesia was similar to the others because performing dental treatments was more difficult in these patients and oral hygiene was worse. Very few patients were under general anesthesia, but the highest complication rates occurred in this group.
All syndromic patients showed difficult vascular and airway access due to anatomical deformities [24], which led to a longer operation time in some patients.
In the Group III patients with psychiatric problems, sedation was performed more frequently as compared to the other groups. However, general anesthesia/sedation rate was higher as compared to the other groups. The most commonly used sedation combination was midazolam, propofol, and ketamine, similar to other groups. A study by Kaviani et al. [25] reports successful results with fentanyl and ketamine combined with midazolam. All patients were subjected to an outpatient treatment protocol. Secondary disease originating from the central nervous system was seen in 69% patients. The number of male patients was higher in all groups, except in Group IV. However, the number of male patients in this group was more than twice that of females. We observed that anxiety and dental phobia were more common in male patients [26].
Group IV comprised of physically disabled people. The mean age and duration of anesthesia was the least in this group. These patients had lesser dental problems because they were young, and without mental problems or secondary diseases. Almost all patients underwent sedation without complications. Because they did not have a disease other than the primary disease and had shorter anesthesia duration, the complication rate was low. Midazolam and propofol drug combination was most commonly used in these patients. We believe that this combination is more effective for short-term sedation and this is supported by literature [27].
Patients with complex medical history were included in Group V, which showed longest duration of anesthesia and highest mean age. General anesthesia was performed the most in this group. The occurence of more than one systemic disease was more prevalent in this group than in the other groups, except in Group I. The preference for general anesthesia is directly associated with the duration of the procedure, longer the procedure, greater the need for general anesthesia. Nasal intubation is indicated if there is no contraindication to the oral procedures [28]. Because anatomic airway problems were expected in these patients, nasal intubation was not used much. Most inpatient treatments were performed in this group. The duration of the procedure, preference for general anesthesia, as well as accompanying secondary diseases increased the need for inpatient treatment and follow-up. Maximum number of sedation drugs was used in this group, because the complex medical conditions of these patients made it necessary to combine different drugs. Literature reports that combinations of sedative agents can be administered to avoid depression of respiration [911].
Pentothal was more preferred in general anesthesia induction in all the groups, because of the high number of epileptic patients. There are studies in the literature reporting the successful application of nitrogen protoxide in conscious sedation of pediatric patients [29]. However, nitrogen protoxide was not used in any groups in our study, because airway problems could have been an issue in each group.
Local anesthesia is sufficient for simple dental treatments, and 90% of the patients in our study sustained with it, but some patients (7%) needed additional analgesia. Narcotıc analgesics were administered in operations causing severe pain (3%). Özkan et al. [30], in their study of narcotic analgesic requirement in dental treatment 3% as stated in the literature.
The literature concludes that dental treatments for PSHCN should be performed under general anesthesia or sedation [31323334]. However, the anesthetic methods and approaches used are not mentioned, thus our publication is a first in this respect. There have been no studies evaluating these parameters to report in this section. Hence, we found it appropriate to evaluate and compare our groups amongst themselves.
Therefore, these procedures can be performed safely with detailed preoperative examination, appropriate premedication and anesthetic agents, selection of method and equipment, and experienced staff. In our study, the expected complications were not as severe as reported in the literature, because conditions were maintained at an optimum level.
 XML Download
XML Download