

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Schwannomas are slowly growing nerve sheath tumors, and can arise from any nerve containing Schwann cells [1]. However, schwannomas at the subfrontal area are rarely reported because the Schwann cell layer lacks in olfactory or optic nerves [12]. Moreover, there are few cases of olfactory schwannomas extending broadly to nasal cavity. We present this unusual case that was treated successfully by gamma knife radiosurgery following surgical excision.
CASE REPORT
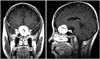
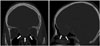
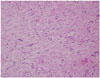
A 51-year-old female patient visited our institution due to anosmia and mild nausea. There was no other neurologic deficit or sign of increased intracranial pressure. Magnetic resonance imaging (MRI) of brain revealed a 3.5 cm-sized subfrontal extraaxial mass resembling an olfactory groove meningioma (Fig. 1). The mass was extended to nasal cavity. Brain computed tomography (CT) scans showed that the anterior skull base had a defect or was very thinned (Fig. 2). We performed a bifrontal craniotomy for surgical excision. We found that the mass was not related to the dura. Both olfactory nerves were compressed by the tumor and displaced to superolateral area of the tumor. The tumor was very hard, therefore was removed in piece. After internal decompression of the tumor, the remnant tumor at the anterior skull base and clinoid process were removed. We tried to find the tumor origin site, but could not. The tumor could not be totally removed, as we wished to prevent a skull base defect. The histopathological diagnosis was schwannoma (Fig. 3). There were no postoperative complications such as cerebrospinal fluid (CSF) leakage. Follow-up MRI at postoperative a day revealed some mass over the distorted anterior skull base (Fig. 4A). The residual tumor was treated with gamma knife radiosurgery one month postoperatively. The marginal radiation dose was 23.5 gray at 50% isodose line. The nasal cavity mass has not grown as of five years after radiosurgery (Fig. 4B).
DISCUSSION
The first consideration in the differential diagnosis of a large and enhancing subfrontal mass in adult is a meningioma [23]. Subfrontal or olfactory groove schwannomas, which are exceedingly rare, are difficult to be distinguished from meningiomas by imaging only [2]. Amador et al. [4] mentioned that the distinction point between schwannoma and meningioma is the adjacent bone state. Schwannomas cause a little more bony erosion, whereas meningiomas tend to cause hyperostosis. In our case, bony erosion and a defect were identified on MRI and CT scans, but we did not expect this tumor to be a schwannoma because subfrontal schwannomas were rarely reported [123]. Neuroblastoma, squamous cell carcinoma, adenocarcinoma, and metastases should be also considered in the differential diagnosis in adults with a tumor involving both the nasal cavity and anterior skull base. These tumors are more aggressive, therefore more extensive resection is required [3].
Total surgical excision is accepted as the best treatment of schwannoma [1]. Subfrontal schwannomas extending to nasal cavity can be treated by total surgical excision with skull base reconstruction [35]. Some authors use transnasal endoscopic resection to remove subfrontal schwannomas extending to nasal cavity with small skull base defect [26]. We planned to treat this tumor by gamma knife radiosurgery following subtotal surgical excision without skull base reconstruction, because the thinned or eroded anterior skull base was very wide. We expected a very high risk of CSF leakage despite skull base reconstruction techniques or sealing products. We performed radiosurgery as planned, because the tumor control rate of schwannoma after radiosurgery is high [78]. There was no complication and the tumor is well controlled as of five years postsurgery.
The olfactory nerve does not have a Schwann cell layer [19]. Therefore, schwannoma cannot arise from this nerve theoretically. There are two types of hypotheses for the origin of subfrontal schwannoma: developmental and non-developmental [19]. The developmental hypothesis suggests an origin from aberrant Schwann cells, multipotent mesenchymal cells, or displaced neural crest cells of Schwann cells within the central nervous system parenchyma. The non-developmental hypothesis suggests that subfrontal schwannomas originate from Schwann cells in the perivascular nerve plexus surrounding cerebral blood vessels, meningeal branches of the trigeminal nerve, or anterior ethmoidal nerves innervating the anterior cranial fossa [19]. Adachi et al. [10] proposed another classification of subfrontal schwannomas according to location of origin: the olfactory site (from olfactory groove or cribriform plate) or others (from non-olfactory sites). In our case, we could not confirm the origin of the subfrontal tumor because of the remnant mass over the anterior skull base.
In conclusion, this is a rare case of subfrontal schwannoma extending broadly to the nasal cavity. We treated this rare tumor by gamma knife radiosurgery following subtotal surgical excision. In general, the best treatment method of schwannoma is total excision. However, radiosurgery following subtotal excision is another good treatment option, if a large skull base defect is likely after total excision of a subfrontal schwannoma.

 XML Download
XML Download