

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Surgical resection is the best management option, in patients with hepatocellular carcinoma (HCC), provided that the remnant liver function is adequate.12 However, intrahepatic recurrence is a major cause of prognosis compromise in HCC, even after liver transplantation.34 Hence, extensive studies have been performed to identify the risk factors that predict HCC recurrence. The studies conducted to date have stratified the patients into recurrent and non-recurrent groups,456 or according to the location of the recurrence (intrahepatic vs. extrahepatic),34 time to recurrence (early vs. late),5789 or number of detected recurrent nodules (single vs. multiple vs. diffuse).101112 The identification of factors related to recurrence is important for predicting the prognosis and for establishing treatment plans.10 However, published factor analysis results are often inconsistent, presumably due to different patient populations and small cohort sizes.
The aim of this study was to identify the risk factors of the intrahepatic recurrence of single nodular HCC, for all recurrences, whether early or multiple, and to compare the results in order to identify the common denominators of poor prognoses. To avoid pathologic uncertainty, we included only patients that underwent surgical resection as an initial management. In addition, the patients were restricted to single nodular HCC at presentation and intrahepatic recurrence only, to avoid confounding variables.13
MATERIALS AND METHODS
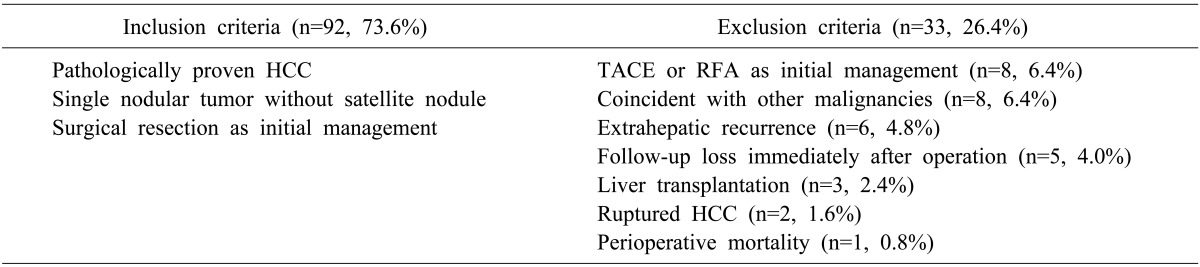
From January 2007 to December 2013, 125 consecutive patients were managed by surgical resection for pathologically proven single nodular HCC at our institution, and all were initially considered for this study, with the follow-up ending on December 31st, 2014. Of these 125 patients, 33 were excluded in accordance with our exclusion criteria (Table 1). Six (4.8%) of the 33 patients had an extrahepatic recurrence, and one patient (0.8%) was a perioperative mortality. Another eight (6.4%) patients were excluded due to a concurrence of combined intrahepatic cholangiocarcinoma.
The medical records of the remaining 92 were reviewed retrospectively, and constituted the study cohort. The operative methods were classified as hemihepatectomy, sectionectomy, segmentectomy (anatomical resection), and tumorectomy (non-anatomical resection). Regarding the pathologic data, the gross type was classified as described by The Korean Liver Cancer Study Group, and the differentiation was determined by the worst Edmondson-Steiner grade.9 Follow-ups were performed at 3 to 6 months intervals, unless a postoperative complication was encountered, or a recurrence was suspected. Follow-up studies and tests consisted of an alpha-fetoprotein (AFP) and a PIVKA (protein induced by vitamin K absence or antagonist), an abdominal computed tomography (CT) and/or magnetic resonance (MR) imaging, as well as a liver function test with coagulation profiles.
Recurrence was defined as the first appearance of an enhancing liver mass, with delayed wash-out, during the follow-up as determined by imaging studies. The patients were divided into recurrent and non-recurrent groups; the recurrent group was further divided into subgroups by applying two criteria: namely, early or late recurrence, and single or multiple recurrences. Early recurrence was defined as the detection of the first recurrence within 18 months of surgery, which was approximated as the mean recurrence-free period (RFP) of all recurred patients. A risk factor analysis was performed to investigate the effect of time-to-recurrence by re-performing the analysis for a RFP of 10 months (the median RFP of all recurred patients). Multiple recurrences were defined as the detection of two or more recurrent nodules, or diffuse recurrence at first detection. Similarly, the analysis was re-performed by dividing the recurrent group by the nodule number, using cutoffs of 1 (single vs. multiple) or 3 (fewer, ≤3 vs. diffuse, >3) to determine whether the choice of cutoff affects the results of the risk factor analysis. A clinicopathological factor analysis was performed using the Student's T-Test, the Chi-Square Test, or Fisher's Exact Test, as appropriate, to compare the groups. A multivariate analysis was performed using the Cox proportional hazard model for recurrence, to determine the statistical significances of factors identified by the univariate analysis, and a logistic regression analysis was used to identify factors associated with early and multiple recurrences. Median RFPs were calculated using the Kaplan-Meier method, and a factor analysis was performed using the log-rank test. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp. Armonk, NY, USA), and the p-values of <0.05 were considered statistically significant.
RESULT
Patient characteristics
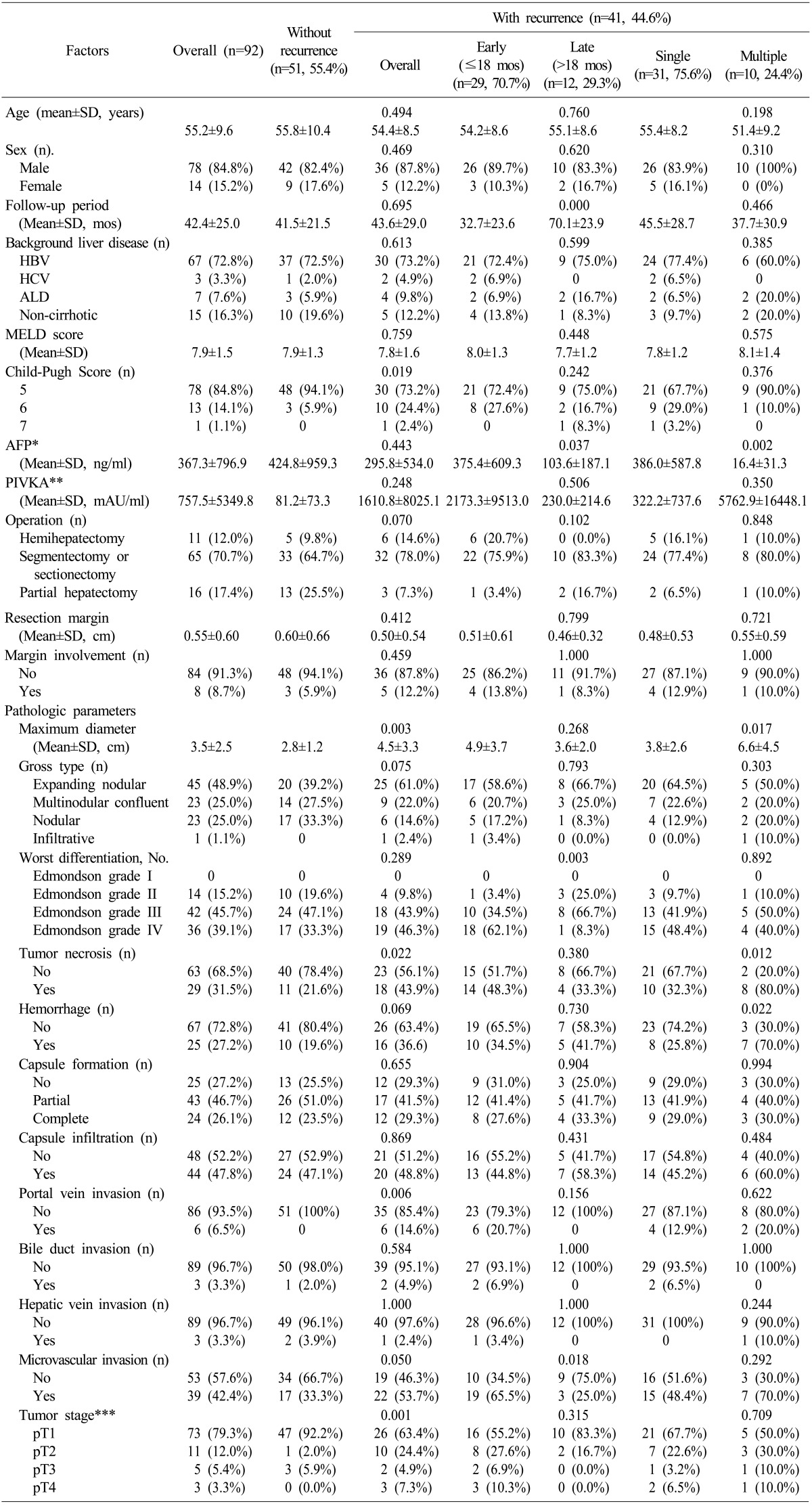
The demographic data and clinicopathological parameters of the 92 patients are presented in Table 2. The overall mean patient age was 55.2 years, and there were 78 men and 14 women (a male to female sex ratio of 5.6:1). The most common cause of background liver diseases were hepatitis B infection (n=67). In contrast, 15 patients (16.3%) had non-cirrhotic livers. In 76 patients (82.7%), one or more liver segments were resected, and in 16 patients (17.4%), only the HCC mass was removed by way of partial hepatectomy, with as much safety margin as possible.
Risk factor analysis for tumor recurrence
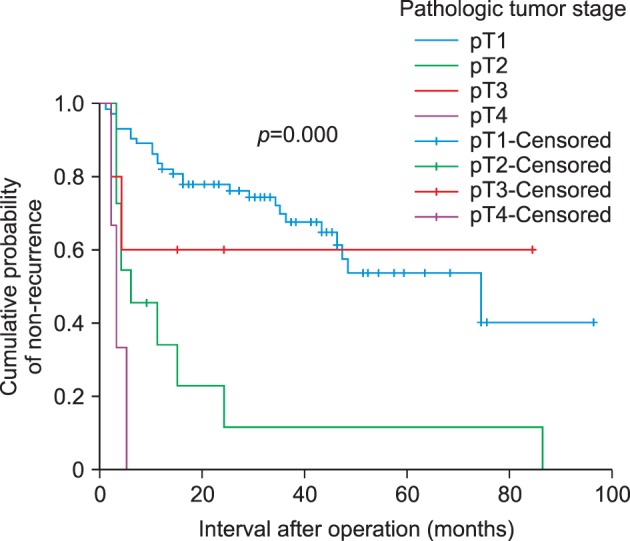
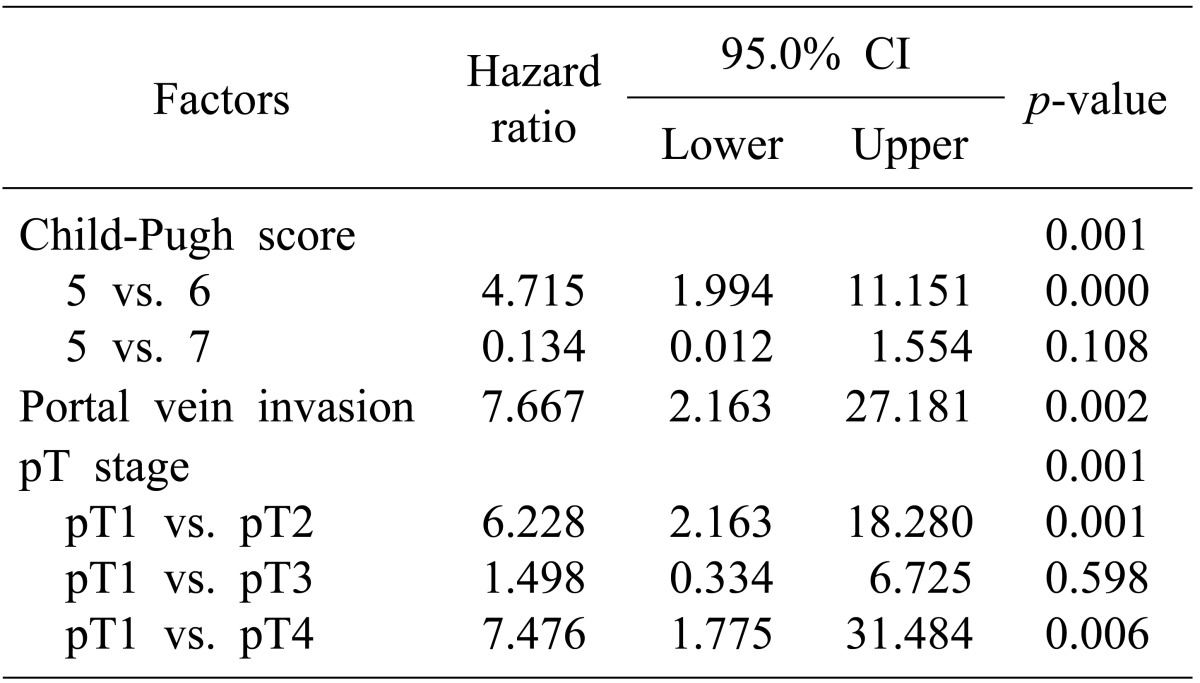
Over a mean follow-up of 42.4 months, 41 patients (44.6%) were found to have an intrahepatic recurrence of HCC (Table 2). The mean follow-up periods in the non-recurrence and recurrence groups were not different (41.5 vs. 43.6 months, respectively, p=0.695). Of the parameters tested, the Child-Pugh score (p=0.019), the maximum tumor diameter (p=0.003), tumor necrosis (p=0.022), portal vein invasion (p=0.006), and pathologic tumor (pT) stage [according to the 7th AJCC staging system (p=0.001)] were found to be significantly associated with an HCC recurrence according to the univariate analysis. The multivariate analysis showed that the Child-Pugh score (p=0.001), portal vein invasion (p=0.002), and the pT stage (p=0.001) independently predicted recurrence (Table 3). The RFP curve, according to pT stages, is shown in Fig. 1.
Risk factor analysis for early tumor recurrence
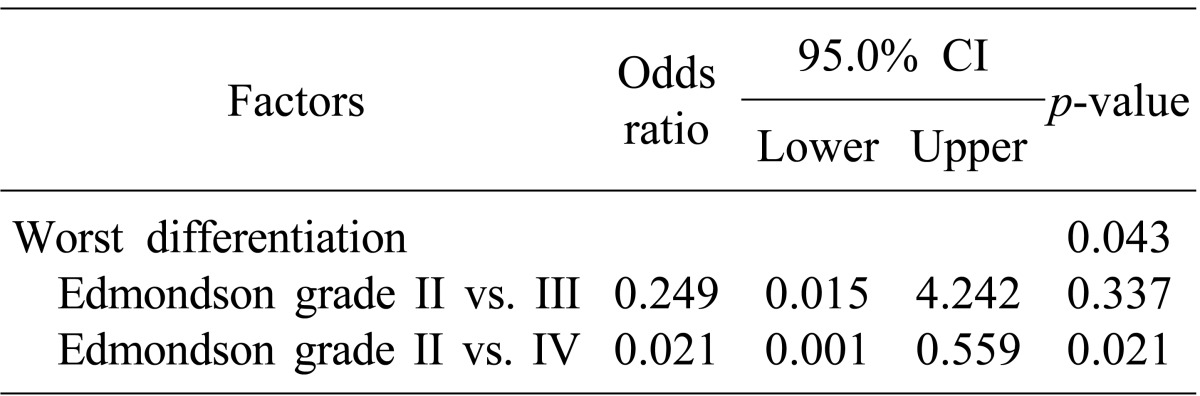
Of the 41 recurred patients, 29 (70.7%) recurred within 18 months. The median RFP for the early recurrence group was 5.0 months (in a range of 1-16 months), and that of the corresponding late recurrence group was 39.5 months (in a range of 24-86 months). The AFP (p=0.037), tumor differentiation (p=0.003), and microvascular invasion (p=0.018) were found to be significantly associated with early recurrence according to the univariate analysis (Table 2). However, tumor differentiation (p=0.043) was the sole independent risk factor according to the multivariate analysis (Table 4).
When the RFP for early recurrence was set again to within 10 months, 21 patients (51.2%) had an early recurrence with the median RFP of 3 months (in a range of 1-10 months), and the median RFP for the late recurrence group was 27 months (in a range of 11-86 months). Differentiation (p=0.004), portal vein invasion (p=0.021), and microvascular invasion (p=0.003) were significant risk factors according to the univariate analysis (data not presented). In the multivariate analysis, tumor differentiation (p=0.038) was also the only independent risk factor.
Risk factor analysis for multiple tumor recurrences
Ten patients (24.4%) experienced multiple recurrences at first detection. According to the univariate analysis, the AFP (p=0.002), tumor size (p=0.017), tumor necrosis (p=0.012), and hemorrhage (p=0.022) significantly predicted multiple recurrence, but the multivariate analysis failed to identify any independent risk factor.
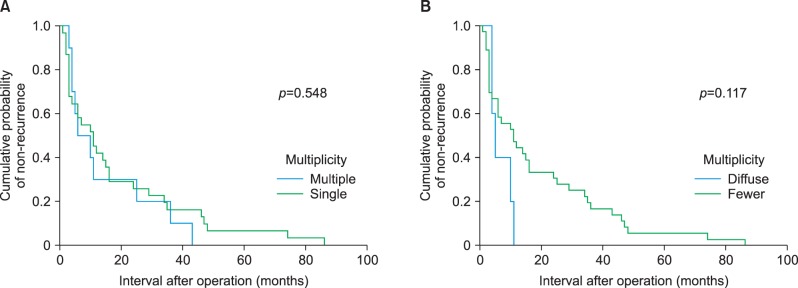
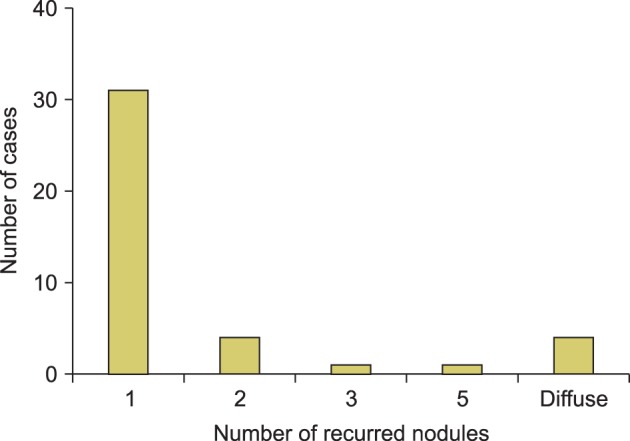
The median RFP for multiple recurrence was 6.0 months (in a range of 3-43 months), while the median RFP for single recurrence (31 patients, 75.6%) was 11.0 months, (in a range of 1-86 months, p=0.584, Fig. 2A). When a cutoff of tumor number 3 was applied, there were 36 patients (87.8%) in the fewer subgroup (nodule number ≤3), and five patients (12.2%) in diffuse (nodule number >3) at first recurrence. A univariate analysis showed the model of end-stage liver disease (MELD) score (p=0.036); the AFP (p=0.003), gross type (p=0.026), and tumor necrosis (p=0.011) were significant risk factors (data not shown), but no independent risk factor was identified by the multivariate analysis. Although the median RFP was significantly shorter in the diffuse subgroup than in the fewer subgroup (5.0 vs. 11.0 months, p=0.003) according to the Student's t-test, this significance was not confirmed by the log-rank test (p=0.117, Fig. 2B). The distributions of the recurrent nodule numbers are presented in Fig. 3.
Comparison of risk factors for tumor recurrence
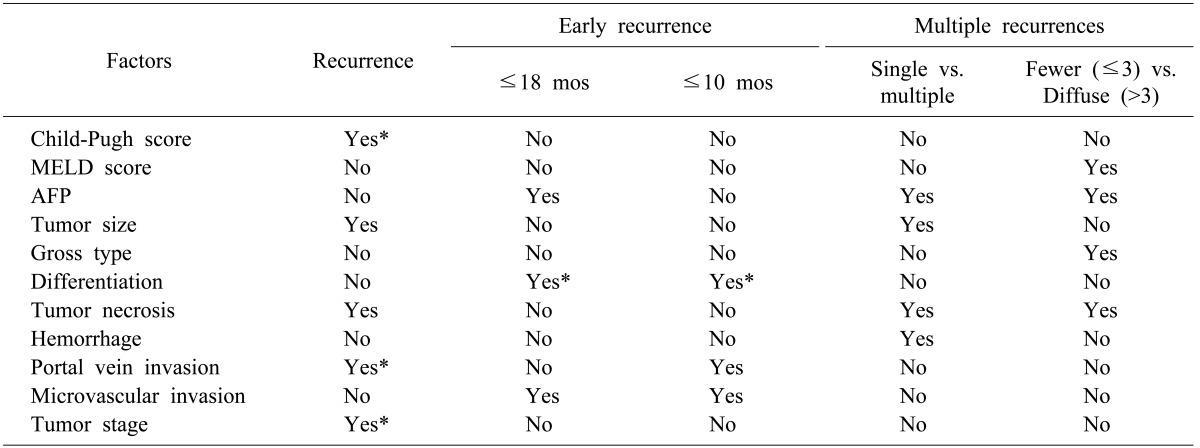
A summary of the risk factors for recurrence, early recurrence, and multiple recurrences are presented in Table 5. No single factor was found to predict the risks of recurrence, early recurrence, and multiple recurrences. Although portal vein invasion was found to be a strong predictor of recurrence, it only predicted early recurrence when a cutoff of 10 months was used. Likewise, although differentiation was found to be an independent risk factor of early recurrence regardless of the RFP criterion, it did not predict recurrence per se, or multiple recurrences. Also, different risk factors were identified by a univariate analysis in each recurrence group, when different criteria were applied. However, no independent risk factor was found to predict recurrence in the multiple recurrence group.
DISCUSSION
Although the prognosis for HCC patients has been improved by the establishment of various management and follow-up strategies, especially those based on considerations of viral hepatitis activity and liver cirrhosis severity, long term outcomes are compromised by intra- and extrahepatic recurrence.514 In this study, the intrahepatic recurrence rate was 44.6%, which is lower than most of those previously reported.35 The possible cause of the lower recurrence rate observed in this study is that macroscopic and microscopic satellite lesions, which are significant predictors of intrahepatic recurrence, were excluded.12
Intrahepatic recurrence has been reported to outnumber extrahepatic recurrence by six to seven fold and,15 thus, intrahepatic recurrence has been the subject of extensive study.5 However, the majority of studies on potential risk factors compared the treatment modalities and/or recurrence patterns, and the reported results vary considerably. Furthermore, the incongruity of the risks identified seems to be due to the different criteria applied, the discriminatory powers of the statistical methods used, and the diversity of the causative agents and patient population.1617 This study shows that changing group criteria, even in the same patient population, results in the identification of different risk factors.4 More specifically, the risk factors of early recurrence were changed by simply modifying the RFP criterion from within 18 months to within 10 months. Likewise, when the recurrence multiplicity cutoff was altered from >1 to >3, different risk factors were identified by the univariate analysis. These results suggest that recurrence, timing, and multiplicity are driven by different factors.5
The tumor size at the initial presentation has been relatively consistently identified as a risk factor of intrahepatic recurrence,418 and this study confirms tumor size as a risk factor along with portal vein invasion, which together constitute the tumor (T) stage as defined by the International Union for Cancer Control (UICC).41920 However, when a risk factor analysis for intrahepatic recurrence was performed versus extrahepatic recurrence, rather than non-recurrence, these significances disappeared.3415 The Child-Pugh score, as an independent risk factor of intrahepatic recurrence, means that liver cirrhosis is a risk factor.4 Cumulative evidence suggests that the primary tumor burden (as indicated by the tumor size and the AFP), as well as the degree of liver cirrhosis (as indicated by the Child-Pugh score and the indocyanine green retention test) are the major conditions that provoke the intrahepatic recurrence of HCC, irrespective of the initial management modality.67212223 Of note, the width and involvement of the resection margins and methods (anatomical resection versus partial hepatectomy), which are long debated issues in the context of recurrence, were not identified as risk factors in this study.1824
When HCC recurrence was subdivided into early and late recurrence, using an RFP cutoff of 18 months, the risk factors identified differed from those of recurrence per se. In this study, tumor differentiation was an independent risk factor of early recurrence for RFP cutoffs of 18 and 10 months, and tumor differentiation is known to be related to tumor invasiveness;15 however, tumor size and portal vein invasion were not found to be risk factors, even by the univariate analysis. On the other hand, Shirabe et al.8 reported that capsule invasion, a tumor location deep in the liver parenchyma, and portal vein invasion independently predicted early HCC recurrence. These discrepancies between the identified risk factors may be due to the definitions of early recurrence used, and the different study populations.25 Although the term 'early' is non-specific, discrimination is required to define the timing of recurrent HCC, because synchronous metastasis has a poorer prognosis than metachronous occurrence.26 Some authors have defined synchronous and metachronous recurrences, using modes of recurrence like intrahepatic metastasis and multicentric occurrence, respectively, and not time courses.27 We do not agree with the use of the same definitions for timing and modes of recurrence, and hope that further studies (based on tumor nucleic acid sequencing) contribute to the refining of the terminologies used.28
In our series, the serum AFP level, tumor size, tumor necrosis, and hemorrhage were significant risk factors for multiple recurrence, according to the univariate analysis. When a multiplicity cut off of >3 was used, rather than a cutoff of >1, the MELD score and the gross type replaced the tumor size and hemorrhage. Interestingly, the former factors are related to tumor mass,29 while the latter are indicative of liver cirrhosis and tumor invasiveness, respectively.1230 Our failure to identify independent risk factors in this study may have been due to the limited number of cases, especially in the diffuse recurrence subgroup, but it might also have been due to the complex relationships between the risk factors.31 The distribution of the number of recurrent nodules among the 41 patients had two peaks at one nodule, and for diffuse recurrence throughout the remnant liver. Many authors have set the cutoff number for multiple recurrences to >3 nodules,6101129 and we found that counting more than five nodules is impractical. Whatever number criterion is used to define multiplicity, the presence of two peaks in the nodule number distribution indicates that there are distinct groups with different etiologies and prognoses.111229
There were some limitations to this study. Since this was a small-volume retrospective study reported by a single center, high-volume multicenter studies need to be performed to validate our results. We presented only the recurrence-free survival results in this study, to avoid complexity of data presentation; thus, the overall patient survival results were omitted.
In conclusion, our results imply that different factors can predict recurrence, timing, and multiplicity of HCC recurrence. Further studies should be conducted to prove the complex relationships between tumor burden, invasiveness, and underlying liver cirrhosis of initial tumors, as well as the timing and multiplicity of recurrent HCC.
 XML Download
XML Download