

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The internal jugular vein (IJV), which collects much of the blood flow from the cerebrum and cerebellum, is main cerebral venous outflow tract. Anatomically, IJV immediately below the jugular foramen is located directly above the anterior surface of the lateral mass of the atlas. Depending on the position, the lateral mass of the atlas indents or kinks the wall of the IJV and causing the obstruction (1-4).
We have observed that the asymmetric obstruction of IJV is occasionally identified in patients who underwent contrast-enhanced MR angiography (CE-MRA). However, it remains unclear whether the asymptomatic obstruction is associated by thrombosis or by secondary compression, Thus neck contrast-enhanced computed tomography (CE-CT) was used for evaluation of the internal jugular vein and surrounding bony morphology. The purpose of our study is to evaluate the cause of high level IJV obstruction on head and neck CE-MRA and CE-CT.
Materials and Methods
Patients
This retrospective study was approved by our institutional review board (IRB), and informed consent was waived.
Head and neck CE-MRA and CE-CT were retrospectively collected from 2005 through 2008 regardless of clinical history. Total 1800 cases of head and neck CE-MRA were reviewed. Finally, thirty patients who performed both head and neck CE-MRA and CE-CT were enrolled in this study. All venous phase images of head and neck CE-MRA were reviewed in terms of the presence of IJV obstruction.
Image Acquisition
The neck CE-MRA was performed with a 3T MR unit (Signa® EXCITE™ 3.0T, General Electric Medical Systems, Milwaukee, USA). Three-dimensional neck MRA was performed for arterial and venous phase imaging with following parameters: repetition time 4900 ms, echo time minimum, a 30×27 cm field of view, image matrix 256×192, flip angle 20°, and section thickness 14 mm. The dose of gadobutrol (Gadovist® ; Schering, Berlin, Germany) was 0.2 mL/kg of body weight. The contrast agent injected with a power injector (Spectris MR Injector®; Medrad, Pennsylvania, USA) at a rate of 2 mL/sec. When the contrast was visually detected in the carotid artery by the technologist on axial plane during injection of the contrast, the coronal 3D gradient echo sequence was initiated; and image acquisition time 2-3 minutes. After acquisition of arterial phase of CE-MRA, venous phase images were obtained. For venous phase of CE-MRA, maximum intensity projection (MIP) images were generated using the commercially available 3D-sofware to evaluate the patency of IJV.
The neck CE-CT was performed using a 64-MDCT scanner (Somatom Sensation 64 VB30, Siemens Medical Solutions, Forchheim, Germany). A total of 100 mL of contrast medium (Optiray 350; Tyco healthcare, Canada) was administered intravenously at a rate of 1.5 mL/sec using a power injector (Stellant, Medrad, Pennsylvania, USA). The scanning parameters were as follows: 750 msec gantry rotation time, 120 kV, 220 mAs, 3 mm slice thickeness, and 1.3 cm table feed per rotation.
Image Analysis
The images were independently reviewed by two radiologists in a blinded protocol.
The presence or absence of the IJV obstruction was determined on CE-MRA. We defined obstruction group which had IJV obstruction and control group which had no IJV obstruction on CE-MRA. Following parameters were measured on axial source data of CE-CT, 1) the diameter of IJV at the level of maximum area of lateral mass of the atlas (Fig. 1a); 2) the distance between the styloid process and ipsilateral lateral mass of the atlas at the level of maximum area of lateral mass of the atlas (Fig. 1b); 3) maximum area of lateral mass of the atlas (Fig. 1c). Each parameter was compared between IJV obstruction side and contralateral normal side in obstruction group, and between IJV obstruction side in obstruction group and mean value of both sides in control group.
All measurements were obtained by manually placing measurements calipers. Millimeter measurements were acquired by using the submillimeter measurement and magnification tools on the PACS workstation (Centricity™ PACS, GE Healthcare, Slough, United Kindom).
Statistical Methods
Continuous variables are presented as means ± standard deviations. The statistical significances for measurements data were examined using a Student t-test between the obstruction group and control group. Pearson's correlation was performed to determine correlation between the narrowest IJV diameter and the narrowest distance from styloid process to lateral mass of atlas, as well as between the narrowest IJV diameter and the maximum area of lateral mass of atlas. All raw data were analyzed by using the SPSS software (version 12.0.1, Statistical Package for the Social Sciences, Chicago, USA).
Results
The obstruction group who had IJV obstruction on CE-MRA was eleven cases (male 5, female 6) (Fig. 2a-d). Their mean age was 55 years (range, 24-76 years) at the time of examination. The control group who had no IJV obstruction on CE-MRA was nineteen cases (male 4, female 15) (Fig. 3a-d). Their mean age was 60.9 years (range, 33-79 years).
In obstruction group, the diameter of IJV at obstruction side was 1.6 ± 1.0 mm and at contralateral normal side was 5.1 ± 2.0 mm on axial CE-CT images. There was significant difference between obstruction side and contralateral normal side with a mean difference of 3.5 ± 1.7 mm (p<0.001). The distance between styloid process and lateral mass of atlas was 4.1 ± 2.1 mm at obstruction side and 7.8 ± 3.0 mm at contralateral normal side on axial CE-CT images with significant difference of 3.7 ± 3.2 mm (p<0.01). Maximum area of lateral mass at obstruction side and contralateral normal side was 103.4 ± 25.3 mm2 and 79.2 ± 21.6 mm2, respectively, which significant difference of 24.2 ± 10.5 mm2 (p<0.001) (Table 1).
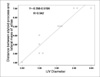
All patients had asymmetry of lateral mass of atlas in obstruction group with significantly larger area at IJV obstruction side than contralateral normal side. The diameter of IJV correlated well with distance between styloid process and lateral mass of atlas (R=0.942, p<0.001) at obstruction side (Fig. 4) in obstruction group. There was no correlation between diameter of IJV and maximum area of lateral mass at obstruction side in obstruction group.
In control group, mean diameter of both IJVs was 5.9 ± 1.6 mm on axial CE-CT and was significantly different from that of obstruction side in obstruction group with a mean difference of 4.3 ± 0.5 mm (p<0.001). The mean distance between styloid process and lateral mass of atlas was 7.7 ± 2.7 mm on axial CE-CT images in control group with significant difference of 3.6 ± 0.9 mm (p<0.001) at obstruction side in obstruction group. The mean maximum area of lateral mass of atlas was 75.1 ± 22.4 mm2 in control group and was significantly smaller than that of obstruction side in obstruction group with a mean difference of 28.4 ± 8.6 mm2 (p<0.05) (Table 2). Each parameter was no difference between the both sides in control group.
Discussion
The use of sitting position during dorsal approach of neurosurgery, turning the head to the side opposite a surgical approach and extending the neck is common practices. During this position, the IJV above the anterior surface of the lateral mass of the atlas on the ipsilateral side of surgical approach cause IJV obstruction (5). Seoane et al. (1) reported compression of the IJV by the lateral mass of the atlas was the cause of cerebellar hemorrhage after supratentorial craniotomy due to neck extension during neurosurgery.
The flow interruption in one IJV at the lateral mass of the atlas with contralateral rotation has been documented angiographically and physiologically in reports dealing with the etiology of tinnitus and cervical venous hum (6, 7). In addition, several studies reported that manual compression of IJV at neutral position resulted in cerebral venous congestion and related to migraine aggravation as well as increasing pressure and volume of the cerebrospinal fluid and especially if it is on the side of the dominant transverse and sigmoid sinuses, may lead to marked increases in intracranial venous pressure (8-10).
Occasionally, IJV obstruction was seen on venous phase of head and neck CE-MRA. However, the cause of IJV obstruction is not certain. We found that IJV diameter and distance between the styloid process and lateral mass of the atlas at the IJV obstruction side in obstruction group were significantly narrower than those of contralateral normal side in obstruction group and mean value of control group on axial CE-CT. The maximum area of lateral mass of atlas at IJV obstruction side in obstruction group was significantly larger than that of contralateral normal side and control group on axial CE-CT. Consequently, IJV obstruction on venous phase of head and neck CE-MRA result from the narrow space between styloid process and lateral mass of the atlas caused by asymmetry of lateral mass of atlas.
These secondary IJV obstruction caused by asymmetry of lateral mass of the atlas should be distinguish from the primary IJV thrombosis and IJV obstruction by invasion from the head and neck malignancies on head and neck CE-MRA. In five cases of control group, IJVs were not interrupted by the styloid process at the level of maximum area of the lateral mass of the atlas. In these cases, the styloid processes were not reached at the level of lateral mass of the atlas and terminated above the level. In four cases of control group, IJVs were not positioned above the anterior surface of the lateral mass of the atlas and they were passed lateral surface of the lateral mass of the atlas without surrounding bony obstacles.
Our study has some limitations that will be overcome in the future. First, we did not evaluate other factors which can induce the IJV obstruction such as rotation, flexion or extension of neck position and angle or length of the styloid process. Especially, posterior deviation of enlongated styloid process may trap the IJV between the styloid process and the lateral mass of the atlas (11, 12). Second, we did not assess the correlation between IJV obstruction and clinical symptom, sign and intracranial pressure. Many patients perform the head and neck CE-MRI and MRA for assessing the cause of neurologic symptoms such as headache and dizziness. In these cases, there are occasionally no abnormality in brain parenchyma and cerebral vessels. Therefore, the association between IJV obstruction by asymmetry of lateral mass of the atlas and neurologic symptoms should be evaluated because it could be one of the cause of neurologic symptoms.
In conclusion, we found that the cause of high level IJV obstruction on head and neck CE-MRA could be narrow space between the styloid process and lateral mass of the atlas, which was related with asymmetric larger area of lateral mass of the atlas.





 XML Download
XML Download