

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cerebral venous sinus thrombosis (CVST) is a rare occurrence during pregnancy and the postpartum period.1) Patients generally have symptoms like seizures, headaches, and other neurologic deficits. These symptoms transpire because of obstruction of cerebral venous sinuses, and decreased drainage of cerebrospinal fluid, leading to intracranial hypertension.2) Early diagnosis and treatment of CVST, which is potentially fatal, are quite important. Pregnancy and puerperium are known CVST risk factors.
Here, we report the case of a young woman who developed CVST two days after normal vaginal delivery.
Case Report
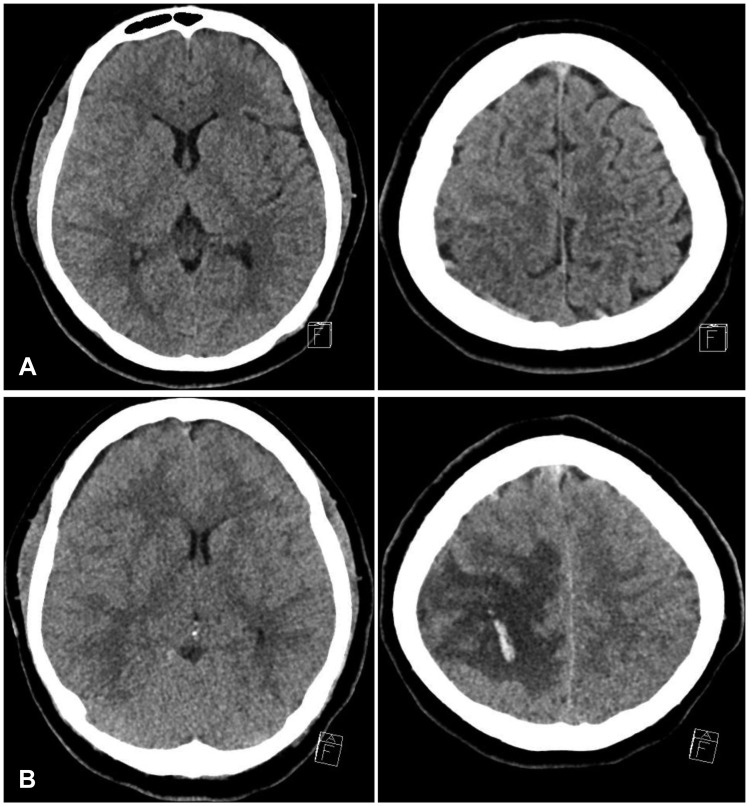
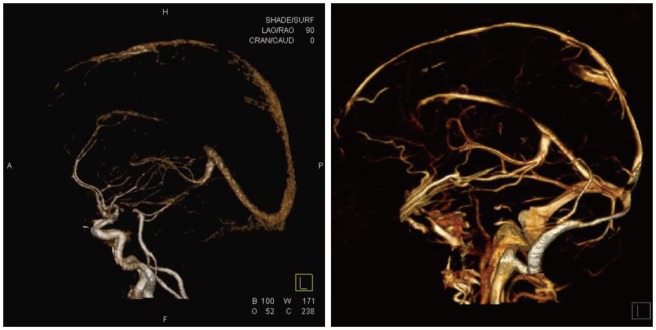
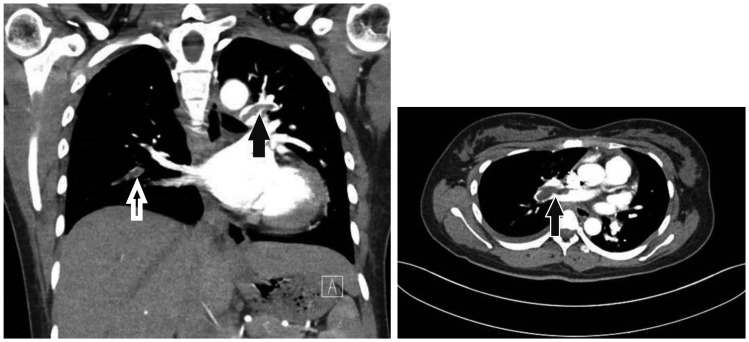
A 20-year-old woman, primigravida, presented with a headache and seizures two days after normal vaginal delivery. She had no past medical history, and no family history of hematological disorder. The seizure was generalised tonic-clonic seizure, and stopped spontaneously after two minutes. She felt an intense headache and had a seizure. After postictal state, her body temperature, heart rate, and blood pressure were 37℃, 88 beats/min, and 130/80 mmHg, respectively. Neurological deficits were not identified. Initially, brain computed tomography (CT) revealed subarachnoid hemorrhage (SAH) in the right parietal lobe and sylvian fissure, and mild cerebral edema (Figure 1A). Considering the patient's age, and absence of a past medical history, brain CT angiography was performed to rule out diseases such as cerebral aneurysm, arteriovenous malformation, or sinus thrombosis. We found a superior sagittal sinus thrombosis. Multiple micro-infarctions were seen on diffusion magnetic resonance (MR) imaging (MRI). Sinus thrombosis was treated with conservative medical treatment, including immediate intravenous administration of heparin and mannitol, as well as blood pressure maintenance. Cerebral digital subtraction angiography was planned to identify definite etiology. Two days after treatment was initiated, patient showed a sudden neurological deterioration, with left side hemiplegia. At the time, she had not been experiencing seizures or a headache. Her consciousness level was E2V3M5 on the Glasgow Coma Scale (GCS). Brain CT showed moderate brain edema, with hemorrhagic densities and midline shift (Figure 1B). Emergency surgical decompression with duroplasty was performed. After the operation, intracranial pressure was controlled using mannitol. To address CVST, systemic heparinization was restarted on post-operative day (POD) 1. On POD 9, the patient's mental state was improved from stupor to drowsy, but left side hemiplegia persisted. Brain CT angiography showed a decrease in size of the superior sinus thrombosis (Figure 2). On POD 28, she developed chest pain. Chest and lower extremity CT angiography was performed to rule out conditions such as deep vein thrombosis and pulmonary thromboembolism. We found a pulmonary thromboembolism at the pulmonary trunk bifurcation (Figure 3). After consultation, we changed the patient's medication to dabigatran (pradaxa). On POD 58, brain swelling reduced, and cranioplasty was performed. Finally, she recovered to E4V5M6 on GCS, and was discharged from hospital.
Discussion
CVST is rare in developed countries, with an incidence rate ranging from 1:10,000 to 1:25,000.1.8) There are no specific symptoms for CVST. Diagnosis is very difficult owing to the condition's rarity and the obscurity of symptoms. Of help, is to note a patient's background and history. Risk factors easily identifiable from a medical history include, pregnancy, puerperium, connective tissue disease, malignancy, contraceptive use, and infections such as, sinusitis, otitis, and mastoiditis.7) Young individuals, especially young women, are more vulnerable. The International Study on CVST reported that 78% of all cases were aged less than 50 years, and that the incidence of CVST was three times greater in women than men.3) When a young, pregnant, or postpartum woman presents with new onset, stroke-like symptoms, such as headaches and seizure, it is significant to examine for the CVST risk factors. If CVST is suspected, CT venography or MR venography should be performed. However, due to its small size, CVST is hard to detect using these conventional modalities. A recent study proved that T2*/susceptibility-weighted MRI sequences are very effective in detecting such lesions. Treatment for CVST is still controversial; however, heparin has been reported as a safe and effective treatment. This is true even when CVST is accompanied by hemorrhagic lesions. Anti-seizure medication should be given to those who present with early seizures. Anticoagulation therapy for CVST averts aggravation of the thrombus, and allows for improvement of the occlusion lesion. This therapy is supported by European Federation of Neurological Societies guidelines. However, in cases of hemorrhagic presentation, appropriate therapy is highly controversial. It has been reported that 39% to 41% of CVST patients present with intracerebral hemorrhage, hemorrhagic venous infarcts, or isolated SAH.4) Although heparin and warfarin have been used for more than 50 years, newer oral anticoagulants (e.g., dabigatran, rivaroxaban, apixaban) might offer an alternative to traditional therapies for CVST, and pulmonary thromboembolism.5)
It is reassuring that although CVST is more usual in connection with puerperium than in the ordinary people, it also has a more favorable outcome. The mortality rate of CVST for all causes is 2% to 10%, but this is noteworthy lower in the puerperium population.6) This case emphasizes the importance of preserving a broad differential diagnosis in women presenting with postpartum seizure. Although eclampsia is the most reasonable cause, other rare conditions, that require decidedly different management, may be responsible.
Conclusion
Here, we presented an extremely rare case of a postpartum patient with CVST. The patient was successfully recovered with surgical decompression and anticoagulants. CVST should be considered in pregnant and young women. Superior sagittal sinus thrombosis is an uncommon complication with an unfavorable outcome after delivery. Timely diagnosis and treatment seem to be important in preventing deterioration of neurological function.
 XML Download
XML Download