

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Internuclear ophthalmoplegia (INO), is caused by lesions in the medial longitudinal fasciculus (MLF), and is characterized by paresis of adduction of the lateral gaze with horizontal jerk nystagmus in the contralateral abducting eye. Although several traumatic INOs have been reported in the literature, it is difficult to radiologically confirm INO when the lesion is tiny. This report presents a case of traumatic unilateral INO due to a tiny hemorrhage at the pontomesencephalic junction diagnosed using susceptibility-weighted imaging (SWI).
Case Report
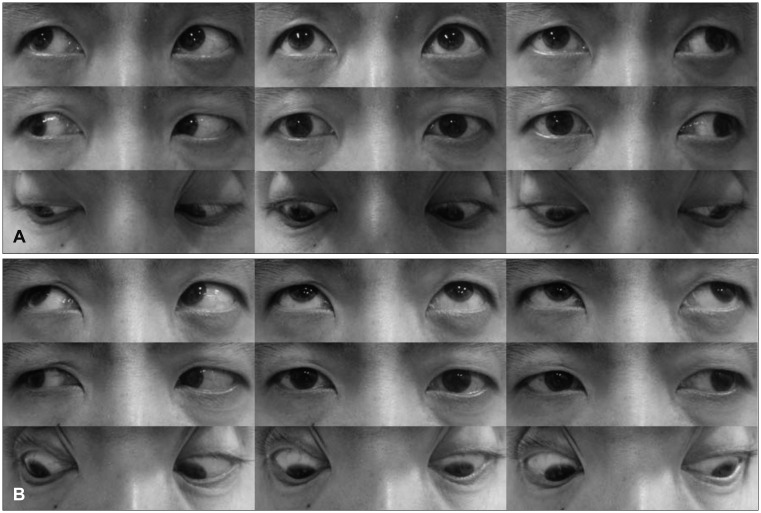
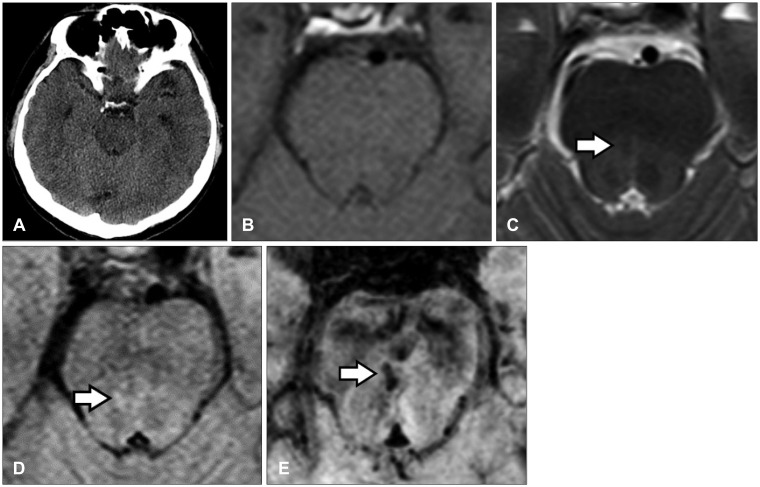
A 43-year-old man was admitted to our neurosurgical department for head trauma after falling backward. The patient had an occipital scalp laceration, brief loss of consciousness with retrograde amnesia, headache, dizziness, and diplopia with left gaze limitation of the right eye. Paresis of adduction of the lateral gaze in the right eye with horizontal jerk nystagmus in the contralateral abducting eye was observed during the neurologic examination at admission (Figure 1A). Initially, brain computed tomography (CT) performed in the emergency department revealed no specific finding (Figure 2A). However, 16 hours after injury, brain MRI showed a faint signal change in the right midline pontomesencephalic junction (Figure 2B-D). Eventually, SWI was performed, which definitively demonstrated a tiny hemorrhage (Figure 2E). Within 12 weeks, the patient's gaze abnormality was fully resolved, and patient reported no subjective complaint of diplopia (Figure 1B).
Discussion
The ocular motor abnormalities of the present patient were consistent with unilateral INO. The most common cause of unilateral INO is a small paramedian pontine infarction, whereas the most common cause of bilateral INO is demyelinating plaque associated with multiple sclerosis.1415) Occasionally, INO is an unexplained consequence often associated with mild head injury.236)
The paramedian pontine reticular formation allows a horizontal conjugate gaze by simultaneously innervating the ipsilateral lateral rectus through the abducens neurons and the contralateral medial rectus through the fibers that originate in the ipsilateral internuclear neurons of the abducens nucleus and cross to traverse the MLF on the opposite side. A lesion in the MLF results in paresis of adduction of the lateral gaze.
The pathogenesis of the isolated damage to the MLF associated with head trauma is unclear, but several mechanisms have been suggested. Common hypotheses on the anatomical origin of post-traumatic MLF injury include differential displacement of the brainstem with resultant stretching of the MLF fibers,12) shearing forces in the brainstem caused by a blow to the head,8) and shearing forces caused by the angular acceleration or deceleration of the head upon impact.10) The shearing forces generated by angular movement exert the maximal effect where the difference between the densities of the cerebrospinal fluid and the adjacent neural tissue is the greatest. Because the MLF is located near the aqueduct and the floor of the fourth ventricle, it is vulnerable to these shearing forces. The posterior portion of the brainstem can be displaced downwardly than the anterior portion because the latter is tethered by small penetrating arteries of the basilar artery.12) Therefore, the shearing forces can create a temporary downward displacement of the posterior brainstem and cause shear injury to the MLF.7) Furthermore, the shearing forces within the brainstem can damage the perforating branches of the basilar artery, resulting in decreased blood flow or focal brainstem hemorrhage.13) In addition, the formation of a subdural hematoma causes a mass effect on the MLF fibers.8)
In most cases, MRI is used to demonstrate the MLF lesion.5111320) Although the standard method to the detect brain hemorrhage is computed tomography CT, but MRI may be as reliable as CT for detecting small hemorrhage associated with trauma.418) But, as we know, conventional MRI can fail to demonstrate a tiny hemorrhage in some patients. If the hemorrhage is very tiny in the brain stem, neuro-images, including brain MRI, may reveal a normal brainstem finding in a patient with traumatic INO.6) Few studies have been conducted in previously documented cases of traumatic INO to correlate structural lesions with possible underlying mechanisms,19) and no previous report had demonstrated microhemorrhage in a traumatic INO case using SWI. The extremely high sensitivity of SWI is particularly suited for the visualization and detection of traumatic hemorrhages, helping correlate clinical findings with the underlying anatomical lesion.1) It uses a high-resolution, completely velocity-compensated, three-dimensional gradient-recalled echo sequence based on both magnitude and phase data. Changes in the signal depend on the paramagnetic properties of deoxyhemoglobin in acute hemorrhage and the intravascular spontaneous blood oxygen-level dependent effect.17) SWI has recently been introduced as a tool to visualize venous vasculature and cerebral microhemorrhages based on the susceptibility difference between deoxyhemoglobin and the surrounding brain tissue.91618)
In this case report, we demonstrated that a traumatic microhemorrhage of the right MLF was responsible for the unilateral INO that presented immediately after head trauma and that SWI was more sensitive than other imaging to identify traumatic INO (Figure 2B-E). It was difficult to identify the cause of the INO using conventional images. T2-weighted, fluid-attenuated inversion recovery image, and isosignal on T1-weighted images showed a faint signal change (Figure 2B-D). But it was difficult to confirm the lesion as a hemorrhage. Eventually, SWI was performed, which showed a prominent hypointense spotty lesion (Figure 2E). As our case demonstrates, the SWI can be useful in precise identification of the anatomical lesions that correlate with the SWI. This technique may improve the diagnostic level of INO by showing greater accuracy for small hemorrhages in the pontomesencephalic junction.
 XML Download
XML Download