

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With advancement in surgical equipments and concern to minimize the surgical invasiveness, burr hole trephination has been the most favorable surgical option in the treatment of patients with chronic subdural hematoma (CSDH).1,2,3,6) In recent times, the majority of these patients have made full neurological recovery after the simple surgical procedures.12) However, skull defects from burr hole trephinations often result in small but undesirable scalp depressions. This undesirable cosmetic defect is often neglected by neurosurgeons because these patients usually recover within short-term hospitalization and follow-up periods, but it is often unacceptable to the patient from a cosmetic perspective. Moreover, the scalp depression aggravates over time with the resolution of wound swelling in the early stage and the atrophy of soft tissue in the late stage, and it can cause a cosmetic complex and functional handicaps to the patients especially during hairdressing or combing.
Whereas a number of reports have discussed cranioplasty to avoid large bone defects, only a few reports have described the problem of small bone defects which, despite their minor size, could result in bothersome cosmetic problems.4,6) To overcome this problem, many materials from bone graft to synthetic materials have been attempted to cover burr hole defect to obtain an ideal cosmetic result, and their clinical results have been evaluated in a few previous studies. These studies usually focused on the biocompatibility, biomechanical strength, or ability of osteogenesis or osteoconduction of the implants, and the cosmetic outcomes were somewhat less emphasized. In addition, there have been no comparative analyses of covered versus uncovered burr holes to demonstrate the efficacy of burr hole covers (BHCs).
Recently, Korean National Health Insurance Service restricted the use of titanium BHC for reconstruction of skull defect after burr hole trephination of CSDH, because effectiveness of this implant has not yet been evaluated well, and the implant at the drainage site may increase the incidence rate of infections, and moreover, simple packing using absorbable gelatin sponge (Gelfoam®; Pfizer Inc., New York, NY, USA) may also have similar clinical outcome.
In order to evaluate the efficacy of titanium BHC after burr hole trephination of CSDH, we compared the degree of burr hole site depressions and complication rates in group with Gelfoam packing only (GPO) and group with reconstruction using titanium BHC, and the cosmetic and functional outcomes were evaluated from patient's aspect.
Materials and Methods
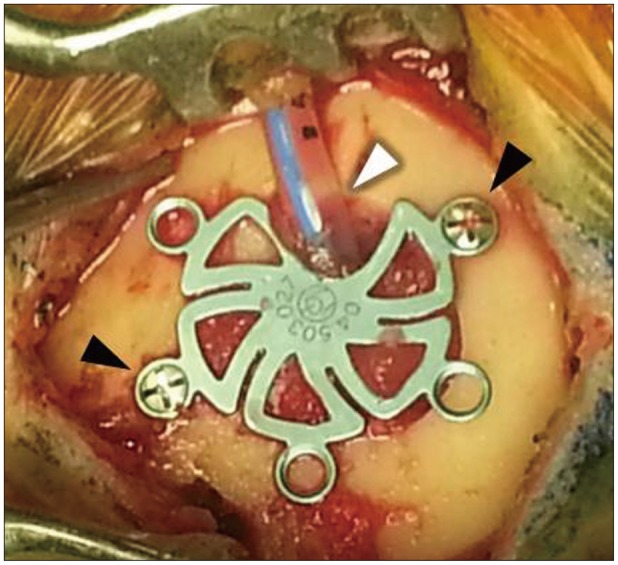
Between January 2009 and December 2013, 230 burr hole trephinations were performed in 196 patients with CSDH at our institute. Their medical records and radiological images were retrospectively reviewed. 34 patients (34 burr holes) were excluded for various reasons; 3 underwent burr hole trephination at the margin of previous craniotomy, 1 was treated using a mesh plate instead of a BHC, 1 underwent another craniotomy for acute subdural hematoma after trephination, and the remaining 29 were lost to the follow-ups. Therefore, overall 196 burr hole cases in 162 patients were enrolled in this study. Patients' profiles, sides of lesions, follow-up periods, modalities of burr hole reconstructions (titanium BHC or GPO), the outcomes such as the presence of scalp depression and the depth of scalp depression, and the complications such as instrument failures or postoperative infections were recorded in detail. These 196 burr holes cases were assigned into two groups; one with GPO and another with reconstruction using titanium BHC. For BHC group, one titanium BHC (Synthes GmbH, Oberdorf, Switzerland) of either 15 mm or 17 mm in size with five screw holes was used depending on the size of defect for each burr hole, and it was fixed using only two or three self-drilling screws. A drainage catheter was located just within the small gap at the edge of burr hole (Figure 1).
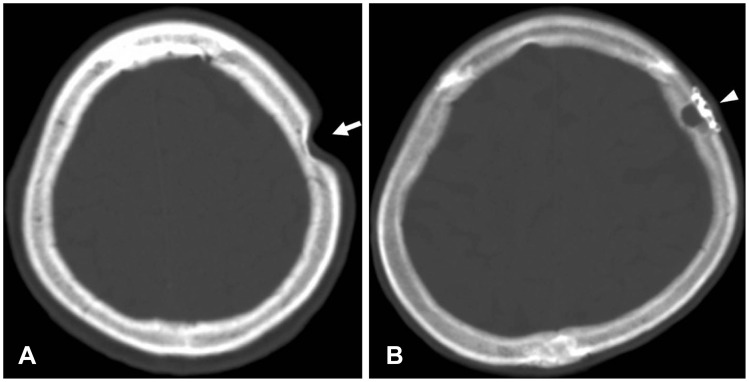
The degree of the scalp depression was measured from the latest follow-up brain computed tomography (CT) using the INFINITT PACS system (INFINITT Healthcare Co. Ltd., Seoul, Korea) in each group (Figure 2). A hypothetical scalp line was drawn by connecting the adjacent normal scalp surface. The depth of scalp depression was measured from this hypothetical scalp line to the deepest point of the depression. In each group, medical records were thoroughly reviewed to confirm the incidence of postoperative infections. Local infections related with operation wound and further disseminated infections such as meningitis or osteomyelitis of skull were included, but infections unrelated with operation site such as pulmonary and urinary infections were excluded. We also searched for occurrence of instrument failures such as screw loosening, displacement of BHC, implant protrusion, or scalp perforation in the worst case from the latest follow-up X-ray and brain CT in the BHC group. In order to evaluate any negative outcomes caused by burr hole defects from patient's aspect, we conducted telephone surveys with the patients who demonstrated scalp depressions on the radiological images, and the respondents were asked to answer whether they had cosmetic inferiority complexes from scalp depressions or functional handicaps during activities of daily life such as hairdressing, combing, scratching scalp, or washing hair.
All acquired data were accurately recorded, and statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 20.0 (SPSS Inc., Chicago, IL, USA). For comparison of GPO and BHC groups, a Student t-test was performed for the continuous variables and Pearson's chi-square for the categorical variables. In all cases, p values of less than 0.05 were considered statistically significant.
Results
Of total 196 burr hole cases, 132 (67.3%) were males and 64 (32.7%) were females. Their ages ranged from 22 to 92 (mean 70.11 years). The mean follow-up period after burr hole trephinations was 20.65 weeks.
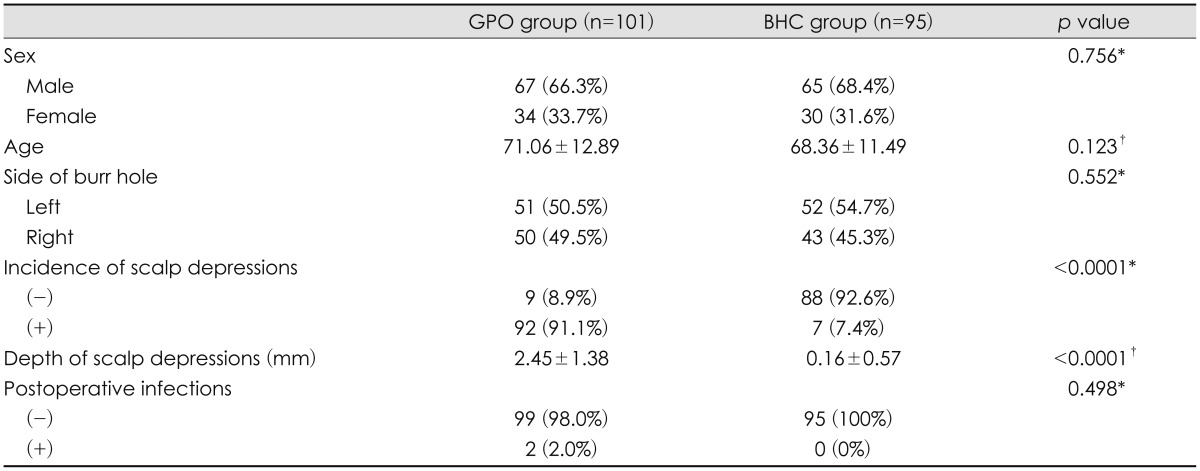
The number of cases in the GPO and the BHC group was 101 (51.5%) and 95 (48.5%) respectively. There were no significant differences in age, sex, and the side of burr hole between two groups. Total 99 scalp depressions were observed after burr hole trephinations; 92 (91.1%) in the GPO group and 7 (7.4%) in the BHC group, and the incidences of scalp depressions between two groups were statistically different based on the results of Pearson's chi-square test (p<0.0001). The mean depth of scalp depressions was 2.45±1.38 mm in GPO group and 0.16±0.57 mm in BHC group, and the difference between two groups was statistically significant based on the result of Student t-test (p<0.0001).
There were two cases of postoperative infections related with operation wound in the GPO group; one was bacterial meningitis and another was local skin infection at operation wound. In contrast, there were no local or disseminated infections related with operation wound in the BHC group in spite of artificial instrumentations. However, these differences between the two groups did not have statistical significance (p=0.498)(Table 1). Any instrument failures such as screw loosening, displacement of BHC, implant protrusion, or scalp perforation were not found from the latest follow-up skull X-ray, brain CT, and medical records in the BHC group.
Telephone surveys were conducted on the 99 patients who demonstrated the scalp depressions on the radiological images. Total 69 patients (69.7%) responded to the survey, and the remaining 30 were excluded because they were out of contact, declined to comment, or died. Seventy-three point nine percent of the respondents said that they had inferiority complexes about cosmetic outcomes from scalp depressions and 62.3% said that they experienced functional handicaps during activities of daily life. In GPO group, 49 (76.6%) of 64 respondents had cosmetic inferiority complexes and 41 (64.1%) experienced functional handicaps whereas, in BHC group, 2 (40.0%) of 5 respondents had cosmetic inferiority complexes and 2 (40.0%) experienced functional handicaps (Table 2).
Discussion
It is well known that burr hole trephination is a simple and effective surgical option to treat patients with CSDH and the rate of its surgical complication is very low.1,2,3,6) However, this small trephination leaves a focal bony defect which eventually causes an undesirable scalp depression. While many neurosurgeons are less concerned about the outcomes of such small scalp depressions, majority of patients experience cosmetic complexes and functional handicaps from these deformities as shown in this study.
Numerous materials have been described to repair bony defects.6,14,15,17,23,24) These implants include organic substitutes such as autologous bone, muscle, or fat tissue, synthetic substitutes such as polymethyl methacrylate (PMMA), hydroxyapatite (HA), or polyethylene, and metallic substitutes.23,28) Organic substitutes are highly biocompatible, but related with donor site complications, time consuming, and difficult to apply. PMMA can be easily applied, but it is time consuming and has thermal reaction which is toxic to surrounding tissues. Mineral graft such as HA is not toxic to the tissues and has osteoconductive properties, but it is too brittle and its resorption easily takes place when cerebrospinal fluid or water is present.9,13) Polyethylene is biocompatible, available in various sizes, and easy and quick to apply. However, its poor cost-effectiveness can be a disadvantage.18,20) Finally, titanium, one of metallic substitutes, has been used in orthopedic, plastic, and maxillofacial surgery in several decades as an alternative to autologous bone because of its good biocompatibility and lack of magnetic properties. It offers greater strength and protection than any other materials. Compared to other metals, it is nontoxic and compatible with surrounding tissues, has extremely low rate of corrosion, and elicits no inflammatory reactions.8,19) In addition to its excellent biocompatibility, BHC made of titanium is magnetic resonance imaging (MRI) compatible and does not produce significant artifacts on CT or MRI.5,7,8,25) Titanium BHC is commercially available in various sizes and shapes, easy to handle, and considerably less expensive than most other substitutes.16) Ones used in this study have five screw holes around and they can be fixed in place using only two or three self-drilling screws in a minute. Different from other types of implants, these titanium BHCs have a small gap or opening at the edge that allows installation of a drainage catheter. This unique feature makes titanium BHC more useful than any other alternatives because insertion of drainage catheter and reconstruction of burr hole defect can be achieved in a single session of operation (Figure 1).
Our study clearly demonstrated much lower incidence of scalp depressions in the BHC group than GPO group. Moreover, GPO group led to deeper scalp depressions than BHC group. In fact, scalp depressions after reconstruction using titanium BHC was almost negligible in most cases (Figure 2). Therefore, we suppose that GPO is insufficient to prevent scalp depression, and titanium BHC is highly effective in preventing scalp depression after burr hole trephination of CSDH.
According to the previous reports, the postoperative infection rate after burr hole trephination of CSDH was 1.28 to 18%.10,11,21,22,26,27,29) In our study, there were two cases (1.02%) of infection in overall 196 cases. Moreover, there were none in the BHC group. Therefore, we consider that application of titanium BHC at the drainage site does not influence the postoperative infection rates in CSDH.
According to our 95 cases in BHC group, there were no instrument failures such as screw loosening, displacement of metallic materials, implant protrusion, or scalp perforation. In our opinion, the reasons for this result are that the skull is not a weight bearing system and the surrounding soft tissues are healed somewhat rapidly because all the instruments are placed beneath the pericranium. Although it is possible to use five titanium screws for all screw holes, the use of only two or three screws is sufficient to construct a rigid structure (Figure 1).
According to our telephone surveys, 73.9% of respondents with scalp depressions had cosmetic inferiority complexes and 62.3% experienced functional handicaps during activities of daily life. Based on these results, we realized that patients were more concerned about the postoperative deformity than expected. Therefore, neurosurgeons should be aware of not only the neurological outcomes but also the cosmetic and functional outcomes caused by even minor burr hole defects.
The ideal implant should be biocompatible, strong enough to retain its physical shape, easy to handle, quick to apply, and cost-effective. The titanium BHC meets these criteria well. Further detailed studies on newer biodegradable materials with larger series of patients are required for advancement in techniques of cranial reconstruction after burr hole trephination of CSDH.
Conclusion
Titanium BHC is highly effective for reconstruction of skull defect after burr hole trephination of CSDH. It provides excellent cosmetic and functional outcomes by preventing scalp depression from burr hole defect without significant complications such as postoperative infections or instrument failures. Neurosurgeons must be aware of the undesirable cosmetic and functional outcomes caused by such minor cranial defects, and these deformities should be adequately repaired.

 XML Download
XML Download