

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Midline splitting cervical laminoplasty (MSCL) has been considered an effective and safe method for decompressing multisegmental cervical lesions caused by cervical spondylotic myelopathy (CSM) or ossification of the posterior longitudinal ligament (OPLL) as well as for achieving immediate stability of these lesions.4,5)
In the beginning of this procedure, autologous grafts from the iliac crest were used to keep the opened lamina splitted.2) However, pain and discomfort at the donor site of the iliac crest were not uncommon, probably due to injury to the superior gluteal nerve,11) and sunken-down of grafted bone spacer occurred. And then hydroxyapatite (HA) was introduced as a spacer material, but the fusion rate between HA and cervical lamina is not good,9) which may cause sunken-down or pull out. In addition, HA has the higher potency of infection than autologous grafts.7)
In contrast, allogeneic bone grafts can avoid the complications associated with harvesting autologous bone. Allograft materials are obtained from deceased human donors, undergoes rigorous safety screening, and can be transplanted into the patient at the time of surgery. The shape of allografts is well developed and capability to keep splitted lamina also increased.6) However, the fusion rate of MSCL using allogeneic bone spacers has not been studied well.
The purpose of this study was to examine the clinical and radiological outcomes in patients undergoing MSCL using allogeneic bone spacers, especially compared the results between CSM and OPLL.
Materials and Methods
A total of 27 consecutive patients with compressive cervical myelopathy including CSM and OPLL underwent MSCL using allogeneic bone spacers, Allo-Spine® LAMINA SPACER (CG Bio, Seoul, Korea) between April 2012 and September 2013. Of these 27 patients, 10 patients were lost to follow-up. Patients with cervical kyphosis, evidence of cervical instability and serious medical problems were excluded for this surgery.
Therefore, we retrospectively analyzed the outcomes of 17 patients (4 men, 13 women). Mean follow-up duration was 11.3 months (range, 6-19 months). Of these patients, 6 were diagnosed as CSM and 11 as OPLL. Three patients of CSM had myelopathy due to dynamic factor such as fall-down and traffic accident, and the others due to static factor such as soft disc herniation and congenital canal stenosis. Fifty nine spacers were used in total. The numbers and locations of spacers were: 11 at C3 level, 17 at C4, 16 at C5, 12 at C6, and 3 at C7.
A single surgeon performed all laminoplasties. He made gutters at the bilateral laminofacet junctions with a 3 mm diameter diamond type burr, and split the midline spinous process with a 2 mm diameter diamond type burr. The allogeneic bone spacers were inserted between the splitted spinous processes and fixed with 1-0 black silk.
Cervical X-rays were taken preoperatively, immediate post-operatively, and after 3, 6 months. Computed tomography (CT) was performed preoperatively, immediate post-operatively, and after 6 months. Cervical lordosis was defined as the angle between C2 and C7 inferior endplates. Change in overall cervical lordosis was assessed on X-ray images (Figure 1). Spinal canal dimension and anteroposterior (AP) distance between the posterior surface of the vertebral body and the anterior surface of allogeneic bone spacer were assessed on axial CT images, which were measured at the level of the vertebral pedicles.
The primary clinical outcome was the rate of change in the Japanese Orthopedic Association (JOA) scores (0-17) between preoperative and postoperative 6 month period. Recovery from myelopathy at 6 months was calculated using the formula: (6 month JOA score-pre operative JOA score)/(17-pre operative JOA score).
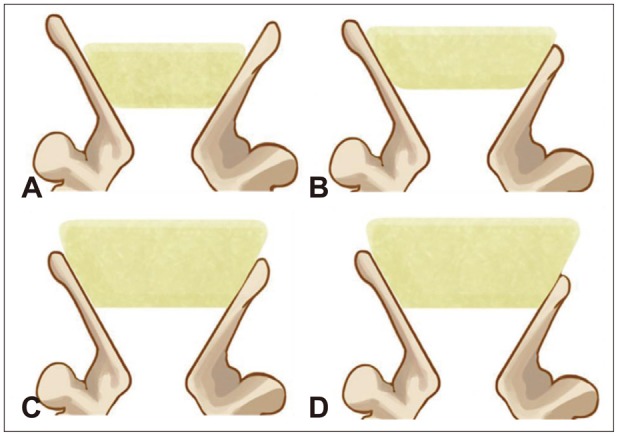
Contact status between lamina and allogeneic bone spacer immediately after surgery, and fusion between lamina and allogeneic bone spacer at 6 months were assayed as Hirabayashi method and Ichikawa classification (Figures 2 and 3).2,3) D or E statuses were classified as fused status.
The factors that affected the rate of fusion between lamina and allogeneic bone spacer were analyzed by uni- and multivariate logistic regression. Age, sex, type of disease (CSM or OPLL), level of operation, contact status, smoking, diabetes mellitus (DM) and hypertension were included in these analyses. Groups were compared using the paired t-test, chi square test, Fisher's exact test, Mann-Whitney test, Linear mixed model, and uni- and multivariate logistic regression. We defined statistical significance as p value <0.05.
Results
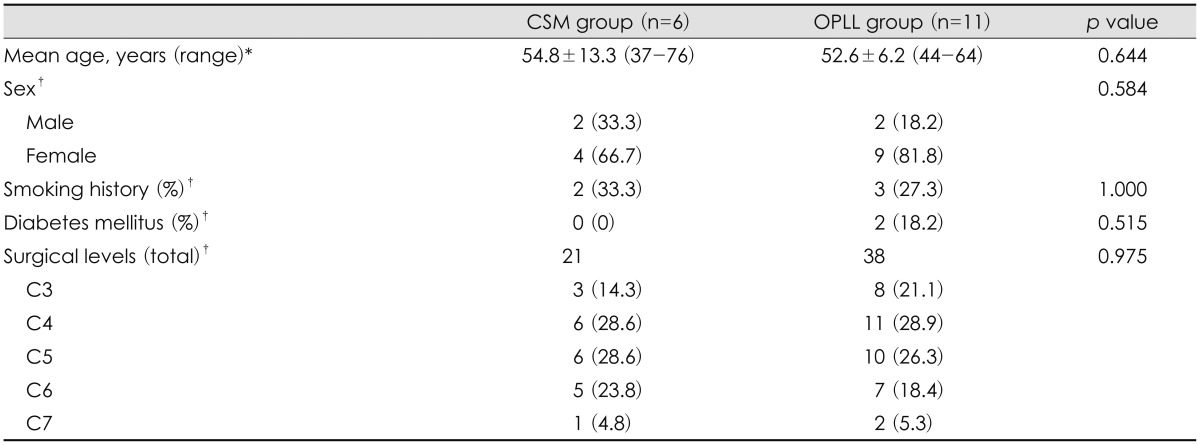
Patients were classified into two groups: CSM and OPLL. The baseline characteristics of the groups are shown in Table 1. Of the 17 included patients, 6 were CSM and 11 were OPLL. Surgeries were performed on 59 levels, 21 for CSM and 38 for OPLL. There was no significant difference between those two groups in baseline characteristics.
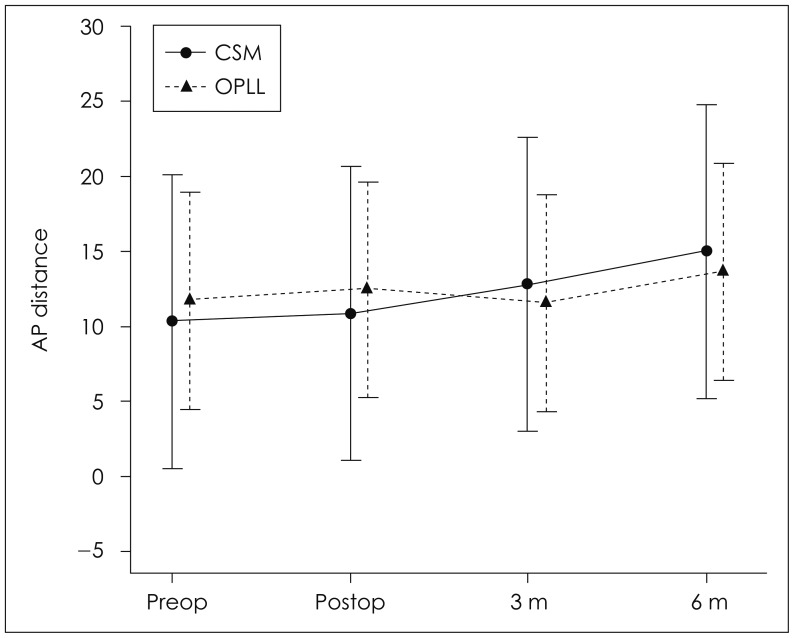
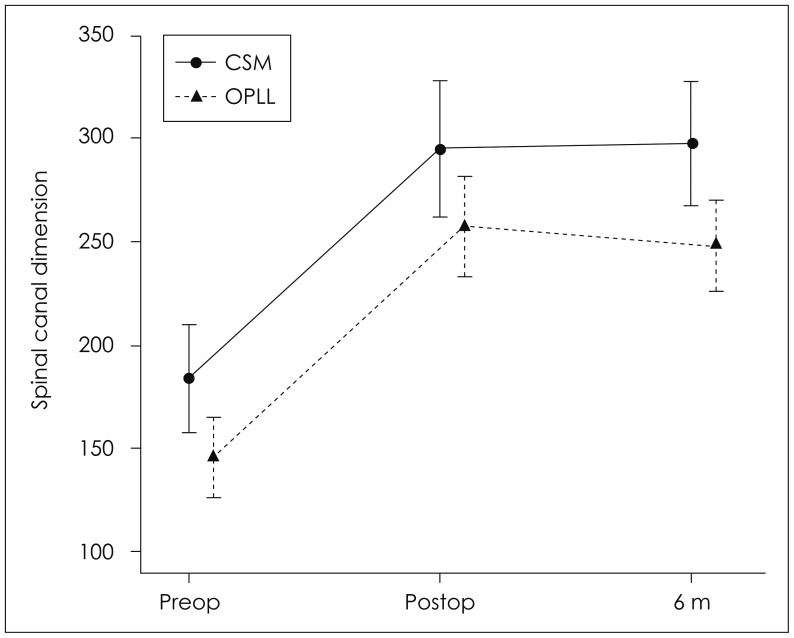
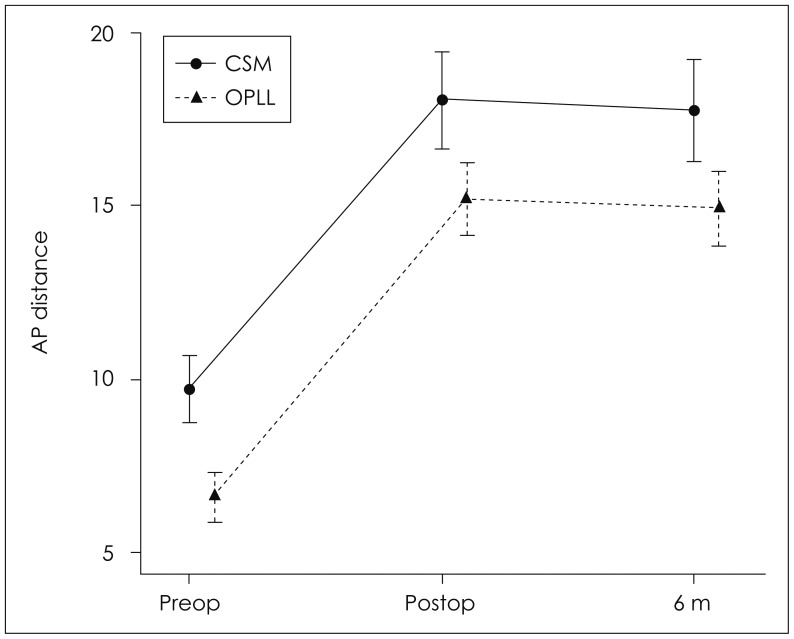
Mean cervical lordosis, which was defined as the angle between C2 and C7 inferior endplates, changed from 10.3±8.7 to 15.0±12.6 degrees in the CSM group and from 11.7±11.1 to 13.6±11.0 degrees in the OPLL group (p=0.602)(Figure 4). These data reveal the mean angle of cervical lordosis was not changed significantly and the occurrence of post-operative kyphosis was negligible. The spinal canal dimension was significantly increased after surgery from 183.1±41.1 mm2 to 295.6±46.2 mm2 in the CSM group (p<0.001) and from 145.5±38.7 mm2 to 255.8±56.6 mm2 in the OPLL group (p<0.001). In addition, the dimensions were evaluated as 299.0±34.2 mm2 (p=0.785) and 248.2±52.2 mm2 (p=0.216), respectively in post-operative 6 months. The spinal canal dimensions were increased with statistical significance after MSCL surgery in both CSM and OPLL, but there was no statistical difference between two groups (p=0.554) (Figure 5). The AP distance of the spinal canal on axial CT images was increased immediately after surgery from 9.6± 1.6 mm to 17.9±2.0 mm in the CSM group (p<0.001) and from 6.5±1.6 mm to 15.0±2.7 mm in the OPLL group (p<0.001), but slightly decreased to 17.7±2.1 mm (p=0.400) and 14.8±2.8 mm (p=0.312), respectively at 6 months (Figure 6). There was also no statistical difference in increase of AP distance between two groups (p=0.924).
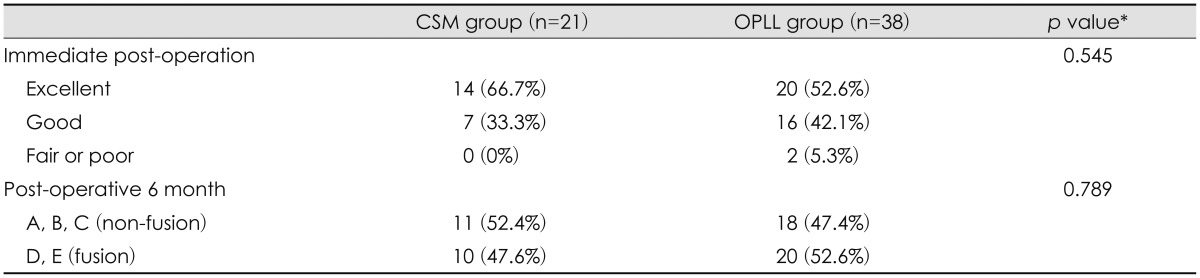
Mean JOA scores changed from 14.3±2.0 to 16.3±0.5 in the CSM group and from 12.0±4.9 to 14.6±2.8 in the OPLL group, with mean calculated recovery rates of 76.4±22.6% and 62.5±27.2%, respectively (p=0.257)(Table 2). There was no post-operative infection.
Excellent contact was achieved with 9.1% of spacers at C3, 35.3% at C4, 81.3% at C5, 100% at C6, and 66.7% at C7 (p<0.001). Contacts between the spacer and the lamina become better in lower cervical level except C7 (Table 3). In the respect of immediate post-operative contact status for CSM and OPLL, excellent in 14 levels (66.7%) and 20 levels (52.6%), good in 7 (33.3%) and 16 (42.1%), and fair at 0 (0%) and 2 (5.3%), respectively (p=0.545). There was no poor status. The post-operative 6 month fusion status between lamina and allogeneic bone spacer, classified as D or E status were 30 (51%) in total, 10 (47.6%) in CSM, and 20 (52.6%) in OPLL (p=0.789). There was no statistical difference in contact and fusion status between two groups. Excellent immediate post-operative contact status between lamina and allogeneic bone spacer had a significantly higher probability of fusion (Table 4). In the respect of immediate post-operative bonding state affecting fusion rate, excellent group showed fusion in 24 (71.0%), good in 5 (22.0%), and fair in 1 (50.0%). Overall fusion rate was 51% (Table 5).
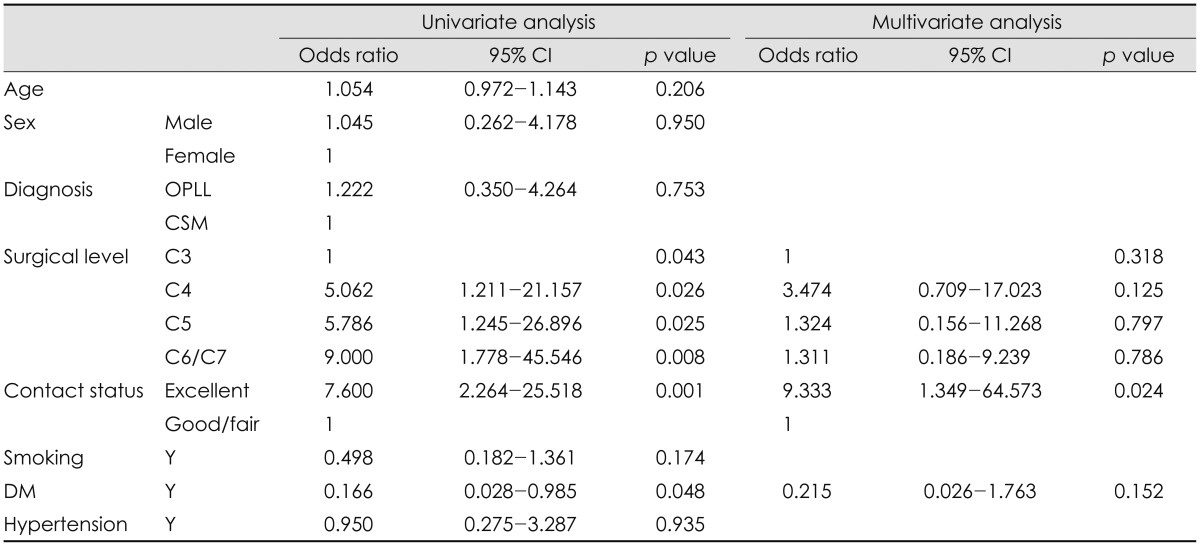
In univariate logistic regression analysis, surgical level of allogeneic bone spacer (p=0.043), immediate post-operative contact status of spacer (p=0.001), and absence of DM (p=0.048) were significant factors. However, multivariate logistic regression analysis showed only contact status of lamina and bone spacer as significant factor of fusion (p=0.024)(Table 6).
Discussion
There was no significant difference in clinical recovery rate between CSM and OPLL in previous studies.1,12) Our results in this present study also support the data, in which post-operative clinical outcomes were significantly improved in CSM as well as OPLL, but no significant difference between two groups. The reason why there was no difference in clinical outcome between two groups could be primarily because this clinical outcome was affected by decompression of the spinal cord and post-operative expansion of spinal canal dimensions were similarly increased in two groups.
In the previous report on MSCL using HA spacer,9) the overall fusion rate between lamina and HA was 27.46% and wingless type HA, which is similar shape as the allogeneic bone spacer used in this study showed 48.8%.9) In our present study, the fusion rate was 51%, which is slightly higher than wingless type HA. Allogeneic bone material has physiologic matrix structure and porosity compared to HA material. Therefore, allogeneic bone spacer seems to have higher potential for bone fusion even though it was sterilized with antibiotics, chemicals, and gamma ray. But it had the potential of disease transmission such as viral hepatitis, tuberculosis, syphilis, septicemia and malignancy.10)
In multivariate analysis, initial contact status between lamina and allogeneic bone spacer significantly affected fusion status. Nagashima et al.8) demonstrated in animal experiments that a high degree of new bone formation occurred at the interface between the spacer and the spinous process. This finding is consistent with our study. We think that the splitted spinous process becomes higher in lower cervical levels and contacts between the spacer and the lamina become better in lower cervical level which explains the significance in univariate analysis.
The limitations of our present study are that this study is not prospective analysis and there were small cases in some classified groups such as C7 level and good/fair contact status. To study further results and outcome about MSCL using allogeneic bone spacer, additive analysis may be needed with prospective, larger cases and longer follow-up duration.





 XML Download
XML Download