

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
1. Necessity of the Research
Humans are continuously exposed to stress and crisis during the changing course of their lives, and must adapt to various roles as required. Individuals may face mental illness or psychosocial difficulties if they fail to respond adequately to the changing environment. Particularly, since Korean university students enter university without considering their aptitude enough due to university entrance examination focused educational environment, they are experiencing difficulty in career and employment problem. In the rapidly changing society and the situation as youth unemployment are adding university students' difficulty more. University period influence the overall occupation of the adults and the social life[1], therefore, it is necessary to adapt to it well.
Although some research has focused on problems with individual fragility, interest has more recently focused on how individuals differ in their capacity to adapt, despite being exposed to similar environments[2]. There has been an emphasis on positive individual qualities, such as hope, optimism, spirituality, and forgiveness, and how these help to promote positive feelings, thoughts, and experiences to enhance happiness and health[3]. During stressful and difficult situations, these positive capacities can elicit positive change, and decrease negative effects; the concept that best represents this is resilience[4].
Resilience research began with studies of children who adapt well even in adversity, and has been extended to adult subjects, and patients. Resilient individuals adapt more effectively to stressful environments and social situations, and are able to recover physically and psychologically[5]. Resilience not only enables children in vulnerable situations to overcome crises and achieve normal growth, but also contributes to a healthy and successful life[6]. Furthermore, resilience is important for health, as it seems to be a protective factor against psychotic symptoms like depression, anxiety, obsessions, and compulsions[7]. Therefore, health professionals, such as nurses, need to consider the resilience.
In Korea, studies on resilience span a variety of fields, such as nursing, medicine, psychology, and pedagogy, but researchers have used different terms for the concept. The concept of resilience is complex and multidimensional., and it is difficult to map its full meaning onto a single Korean word. Furthermore, it is difficult to conduct continuous research, since different researchers use different languages. Thus, Jung and Chae[4] proposed referring to resilience as stress, in accordance with loanword orthography, to reduce the disparity in the understanding of the term, and to facilitate communication among researchers. Since some Korean studies have used the term resilience in accordance with loanword orthography[8,9], this study will use it accordingly.
Although resilience is considered a universal concept [5], it is still poorly understood, as the divergent use of the term in Korea demonstrates. Nevertheless, a better understanding of resilience can inform its clinical and academic application. In addition, precise assessment of the degree of resilience can help to determine the long-term effectiveness of health-associated plans, policies, research, and arbitration[10]. Various tools to measure resilience have been developed and applied, such as the Connor-Davidson Resilience Scale (CD-RISC)[11], the Brief Resilience Scale (BRS)[12], the Baruth Protective Factors Inventory (BPFI)[13], and the Resilience Scale (RS)[14].
In case of Korea, a tool composed of 32 questions targeting university students was developed[1], however it may be difficult to apply in some situations because it contains many items. RS was developed by targeting older adults[14], which is also frequently used in domestic researches. In a literature review of the area, Ahern et al.,[15] rated the RS developed by Wagnild and Young as the best of all resilience tools for young people. The RS is not only applicable across age groups, socioeconomic status, and education level, but it correlates with positive health-promoting factors such as well-being, and with negative factors like stress and hopelessness; it also demonstrates good validity[16]. The RS is a self-report questionnaire developed in 1993; recently Wagnild developed a short version of the RS, the RS-14, to reduce the response burden for survey subjects, and to increase the response rate. There is a high correlation between the RS and RS-14[17]. The RS-14 has been found to be valid and reliable in various countries, such as Japan and China[18,19]; however, it has not yet been tested in Korea. Compared to RS with 25 questions, RS-14 with 14 questions can reduce time on questionnaire, which can be simply applied, so that it can be variously applied for research and working-level. Also, it has an advantage to reduce the object's burden who composes the questionnaire.
Therefore, the purpose of this study is to adapt the RS-14 to Korean university students to verify its validity and reliability. The aim is to confirm the applicability of this tool, thereby potentially contributing to nursing study and practice.
METHODS
1. Study Design
This was a methodological study to confirm the validity and reliability of the RS-14 scale with a sample of Korean university students.
2. Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of the researcher's university (IRB No.: 12-0006). Subjects were given a full explanation of the study purpose and procedures, including issues of privacy, and possible benefits and inconveniences of taking part. Subjects were informed that they could withdraw at any time, and all gave informed consent.
3. Subjects and Data Collection
Subjects were 284 university students. Data was collected from October 1 through December 30, 2012. The researcher and two research assistants explained the self-report questionnaire to subjects and conducted the survey. A total of 273 questionnaires, excluding 11 questionnaires with no responses, were analyzed. Size of sample to verify validity was satisfactory, when standardizing large number among 10 times of 100 and the number of question[20].
4. Study Tools
Wagnild and Young[14] developed the RS in order to measure resilience, and it consists of 25 items. The short form RS-14 consists of 14 items[17]. It uses a 7-point Likert-style scale, ranging from 1 "Strongly disagree" to 7 "Strongly agree." Higher scores indicate higher resilience. The researcher organized the translation and reversetranslation of the scale after obtaining approval from the original author. The translation and reverse-translation were conducted according to the process of translation and adaptation of instruments designated by the World Health Organization.
Professional translators residing in foreign country for 14 years who had earned a degree in English literature in Korea completed the first translation draft. This was then evaluated by three Korean adults for any translation difficulties. The scale was later back-translated by a permanent resident who resided in the USA for 18 years, and who is proficient in English and Korean. The original author then checked this back-translated version. The appropriateness of the terms and items were determined by conducting a pre-test with 10 adults from the target population. Finally, the original author and a professor of nursing evaluated the questionnaire to determine the final version.
5. Data Analysis
SPSS Version 21.0 software was used to analyze the data.
Demographic characteristics were examined using descriptive statistics and percentages.
Principal components analysis was used to generate exploratory factors to determine construct validity.
Criterion-related validity was assessed by examining concurrent validity. Pearson's correlation coefficient was used to confirm the correlation between scores from Radloff's Center for Epidemiologic Studies Depression Scale (CES-D Scale) and Rosenberg's Self-Esteem Scale.
The reliability of the scale was calculated using Cronbach's α coefficient.
RESULTS
1. General Characteristics of Subjects
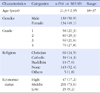
The general characteristics of subjects were as follows: 139 males (50.9%), 134 females (49.1%) out of a total of 273 subjects. The average age was 21.9 and ranged from 18 to 37. There were 58 freshmen (21.3%), 80 sophomores (29.3%), 59 juniors (21.6%), and 76 seniors (27.8 %). In terms of religion, there were 69 Christians (24.5%), 39 Catholics (14.3%), 19 Buddhists (7%), and 143 subjects of no religion (52.4%). All subjects (100%) were single. Regarding economic status, 47 subjects were classed as High (17.2%), 201 as Middle (73.6%), and 25 as Low (9.2%)(Table 1).
1) Adequacy of factor analysis
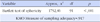
All 14 questionnaires were deemed appropriate for factor analysis, since the Kaiser-Meyer-Olkin (KMO) measure was .917. In addition, Bartlett's test was 1752.86 (p<.001), indicating that the data satisfy the conditions for factor analysis (Table 2).
2. Evaluation of Construct Validity
1) Factor extraction and factor rotation
Since the factors of the original scale were explored using principal components analysis[16], the same method was adopted in this study. The factor analysis results revealed two factors with eigenvalues greater than 1.0, and the scree plot results confirmed two factors. All 14 items showed factor loadings greater than .4 and less than -.4. Factor loadings for Factor 1 were between .48 and .76. Factor loadings for Factor 2 were between .55 and .81. The total variance explained by the extracted factors was 55.4%. The variance explained by Factor 1 was 46.0%, and by Factor 2 was 9.4%(Table 3).
2) Naming factors
Those items that load highly on each factor are assumed to explain more variance[21]; therefore, each factor was named with reference to its highest-loading items. Also, it has appeared as 2 factors in the RS, reflected naming factors and investigation by researcher. In order of high to low loadings, Factor 1 loads items 10, 11, 13, 14, 12, 9, 7, and 4, and Factor 2 loads items 6, 3, 8, 1, 5, and 2. The items loading on Factor 1 relate to trust and confidence in life, and so this factor was named Self-confidence. The items loading on Factor 2 relate to self-control and the ability to manage independently. This factor was therefore named Self-control (Table 3).
3) Verification of independence between factors.
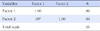
The correlation between the two factors was r=.69 (Table 4). This suggests that the factors were not independent.
3. Evaluation of Concurrent Validity
Rosenberg's Self-Esteem Scale[22], adapted by Jeon [23], was used to verify concurrent validity. The correlation between Factor 1 and self-esteem was r=.45, and between Factor 2 and self-esteem, r=.44. The correlation between the Korean version of the RS-14 and self-esteem was r=.48. The modified and revised Korean version of the CES-D Scale originally developed by Radloff[24], and adapted by Cho and Kim[25] was used. The correlation between depression scores and Factor 1 was r=-.38, and between depression and Factor 2, r=-.45. The correlation between the Korean version of the RS-14 and depression was r=-.44 (Table 5).
4. Evaluation of Reliability
This study confirmed internal consistency reliability for the 14 resilience items (Cronbach's α=.905). For Factor 1, Cronbach's α=.862; for Factor 2, Cronbach's α =.841 (Table 4).
DISCUSSION
The concept of resilience explains how humans exposed to stressful environments can adapt to stress and adversity. A precise measure of resilience is important for providing physical and psychological care in a range of situations. Particularly, Korean university students are experiencing difficulty in career and employment in the rapidly changing society, it is necessary to check resilience for nursing intervention. Compared to RS[14] with 25 questions, which is used in domestic, RS-14[17] with 14 questions has the advantage to simply evaluate resilience within a short time. This study attempted to confirm the validity and reliability of the RS-14 developed by Wagnild[17], to explore its applicability to Korean university students, and verify its possible use for domestic resilience research.
Exploratory factor analysis identified two factors; all items were retained since item loadings were all above .40. Wagnild's research on the original RS-14[17], and work by Nishi et al.,[18] on the Japanese version of the scale, identified one factor, whereas Tian and Hong found two factors for the Chinese version[19], although the items were configured differently to the present study. The two factors on the original RS scale were Personal competence and Acceptance of self and life [14], with items 1, 2, 5, 6, 7, 8, 9, 11, 12, and 14 from the RS-14 loading on Personal competence, and items 3, 4, 10, and 13 loading on Acceptance of self and life. However, in the Korean version of the RS-14, items 10, 11, 13, 14, 12, 9, 7, and 4 load on Factor 1, and items 6, 3, 8, 1, 5, and 2 load on Factor 2. Baek et al.,'s research, which examined the validity and reliability of the Korean version of the CD-RISC, another resilience measure, found factors different to those of the original measure[5]. The differences in factor structure found across studies may reflect cultural differences in the understanding of the resilience concept. A study by Hong[26], which examined the meaning of resilience in Korean cancer patients, identified the following resilience characteristics: self-worth, self-efficacy, self-confidence, independence, optimistic and positive mind, strong will, and responsibility. Hong noted that is reasonable to view that as a result rather than characteristics of resilience to accept and embrace the adversity in life[26]. Although Hong's research was conducted on cancer patients, the concept of acceptance of self and life in Wagnild and Young's research[14] is the results rather than the property of resilience to Koreans. Baek et al.,[5] mentioned that the difference in factor composition in the original tool and Korean tool could appear from the cultural difference, which was influenced by mutually different historical, social, geological environments, etc. The concept of resilience composition should consider social, cultural factors, also, the factors which compose resilience concept may have difference between groups [4]. This highlights the fact that the present study reflects the unique environmental characteristics of Korea.
If we examine the cumulative explanatory power of each factor in this study, Factor 1, Self-confidence, explained 46.02% of the variance, and Factor 2, Self-control, explained 9.40%. The total variance explained by both factors is 55.43%. This is lower than the total explained variance of 61% in Tian and Hong's study[19], but higher than the variance of 39.4% found by Nishi et al.,[18], and the 53% reported by Wagnild[17]. Total variance is used to decide the number of factors long with Eigenvalue. Standard of total variance had difference along with researches, the researcher considers total variance of this research is satisfactory, compared to previous researches.
For factors to be considered independent, their inter-factor correlation must be less than .50. In this study, the inter-factor correlation was high (r=.690). Chung[20] examined the status of validity and reliability research related to the development of measures, there is almost no cases that rarely show correlation since most factors reflect concepts that consist of multiple aspects. All three papers that Chung reviewed showed a significant correlation between factors. The two factors in this research, Self-confidence, self-control, are desirable to be considered as subordinate concepts which compose the concept, resilience, it is considered that correlation between the two factors appeared. Also, it determines a concept by analyzing as one factor in the original tool, it is considered to influence the result of this research. Therefore, each RS-14 Korean version factor can be interpreted as having correlation within the concept of resilience rather than an independent zone.
Regarding concurrent validity, there was a high correlation between self-esteem and depression. Self-esteem is a positive or negative attitude towards the self; a person with high self-esteem respects and values themselves[22]. This study showed a positive correlation between resilience and self-esteem, consistent with previous findings[2,5,18]. Self-esteem is a personal factor that, along with self-efficacy and other personal traits, explains and contributes to resilience[27], and is a key element in enhancing this ability[28]. In the present study, depression showed a negative correlation with resilience, consistent with the findings of Kim and Min[29], who found that resilience correlated highly with anxiety, depression, and alexithymia. Several other studies have reported that depression and resilience are negatively correlated[5,14,18]. A Study by Lee and Kim[1], that resilience displays positive correlation with university life adaptation, besides depression, also supports this research result. This study therefore indicates that the Korean version of the RS-14 has good validity and reliability.
Internal consistency is to check if responses are consistent between several questionnaires in order to verify the same concept, it is determined by α coefficient[30]. This study showed a Cronbach's α of .905 for all items. For Factor 1, Cronbach's α=.862, for Factor 2, Cronbach's α=.841. For the original RS-14 scale, Cronbach's α was .93[17], which is similar to the figure for this study. The α coefficient of reliability can range between 0 and 1, and values between .50 and .80 are considered adequate. The overall reliability, and the reliability for each factor in the Korean version of the RS-14, is high, indicating good internal consistency.
This study has verified the validity and reliability of this adaptation of the RS-14 for use with Korean university students. Therefore, this measure is an adequate tool to assess the degree of resilience; additionally, this shorter version of the scale is more convenient for survey subjects.
One limitation of this study concerns the difference between the present factor structure and those of previous studies. The two-factor structure for resilience in this Korean version of RS-14 needs further investigation using qualitative analysis. It would also be useful to explore further cultural differences in resilience. Previous work indicates that age is an important influence on resilience[18], and Wagnild[17] reports that RS-14 scores increase with age. The average age of the university students in this study was 21.9. Therefore, age may be an influence on the present findings, and this must be considered when using this new version of the scale. There is also evidence that gender affects resilience[2,18], so this needs to be confirmed with the present scale.
Therefore, additional research on this new scale should address several issues. First, the influence of age and gender on resilience needs examining in a Korean sample. Second, the present author is proposing to revalidate this Korean version of the RS-14 for a greater range of subjects, such as patients with chronic disease. Third, this study used a measure designed for use in a different culture, and the present scale is an adaptation for Korean subjects. It is necessary to continue the development of indigenous resilience measures that reflect the characteristics of the Korean culture.
CONCLUSION
This was a methodological study to examine the concept of resilience by adapting the RS-14 to produce a valid and reliable measure to use with Korean university students. The study used a self-report survey with 273 university students, and SPSS Version 21.0 was used to analyze the data collected to verify the validity and reliability of the scale. In order to explore the structure of this measure, principal components analysis was performed, and Pearson's correlation coefficient was used to examine the correlation between this scale and scores from both Rosenberg's self-esteem scale and Radloff's depression measure. Cronbach's coefficient was used to verify the reliability of the scale.
Factor analysis extracted two factors with a total cumulative explanatory power of 55.4%; Factor 1 explained 46.0% of the variance, and Factor 2 explained 9.4%. The correlation between Rosenberg's Self-Esteem Scale and the Korean version of the RS-14 was r=.48 and the correlation between Radloff's depression measure and the RS-14 was r=-.44. The reliability was high (Cronbach's=. 91).
This study demonstrates that the Korean version of the RS-14 has good validity and reliability, and is simple and easy to use; therefore, this scale could make a valuable contribution to resilience research and nursing practice.


 XML Download
XML Download