

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Constipation is a common, chronic digestive disease with a prevalence of 2%–27% in North America [1]. Older people, especially those over 65 years old, have a propensity for constipation and a prevalence of constipation of 30%–40%. Moreover, compared with Caucasian populations, non-Caucasians have 30% higher incidence [2]. Constipation treatment regimens include stimulating laxatives, osmotic agents, diet modifications, and stool softeners [2]. Among these, the stimulating laxative bisacodyl is widely used for both adults and children [3]. The most common side effects of bisacodyl are abdominal pain, diarrhea, and occasionally nausea, headache, and gastroenteritis [34]. No case of proctitis and rectal ulcer after taking oral bisacodyl has been previously reported. We report a case of severe proctitis and rectal ulcers associated with oral bisacodyl, and review the literature.
Case
An 80-year-old woman was admitted to the emergency department because of right wrist pain after a fall. The patient had been diagnosed with Parkinson disease five years previously and was currently taking propranolol 40 mg, levodopa 62.5 mg, choline alfoscerate 400 mg, rebamipide 100 mg, and alprazolam 0.25 mg twice a day. In addition, she had chronic constipation for several years, defecating once every three days. She had no other underlying diseases that might have affected her bowel habits.
The plain radiograph examination showed fractures of right radius, right ulna, and first lumbar vertebra, so the patient was admitted to the orthopedics department. Appropriate splints were applied and the patient was advised bed rest. On the eighth day, the patient complained of a swollen right arm and we administered ceftriaxone (2 g/day) intravenously for cellulitis and its associated pain.
Because the patient was put on absolute bed rest, she complained of aggravated constipation and tenesmus. On the tenth day, oral bisacodyl (5 mg/day) was prescribed and she was recommended to take it daily at bedtime. The patient was unable to defecate even after 6 days of oral bisacodyl; however, on the seventh day after commencing the medication, she began to pass watery diarrhea more than 5 times a day. Despite cessation of bisacodyl and the administration of probiotics, the diarrhea worsened and the patient complained of left lower quadrant abdominal pain and a sensation of chills on the fifth day of watery diarrhea. At the time, her vital signs were stable: blood pressure 171/100 mmHg, heart rate 85 beats per minute, respiration 18 per minute, and temperature 37.7℃. There was no tenderness or rebound tenderness in the abdominal examination. Bowel sounds were somewhat hyperactive. Laboratory testing revealed leukocytes of 9,400/mm3, hemoglobin 12.2 g/dL, platelet count 233,000/mm3, and C-reactive protein 3.04 mg/dL. There were no specific findings on the abdominal plain radiograph. Because it was 14 days after administration of intravenous ceftriaxone, Clostridium difficile colitis was considered, all antibiotics that have associations with diarrhea and colitis were suspended, and oral vancomycin was commenced. C. difficile antigens were all negative in three consecutive stool analyses. White blood cell count in stool was 50–90/HPF. In stool culture, the result was no growth.
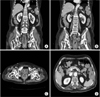
The patient was admitted to the gastroenterology department because of the watery diarrhea, which continued despite the administration of loperamide and suspension of antibiotics. On colonoscopy, multiple 4–5 cm diameter round ulcers were noted at the rectum (5 cm away from the anal dentate line) and a large irregular shaped ulcer was noted at the distal rectum (3 cm away from the anal dentate line) (Fig. 1A, B). The principal pathology findings were neutrophil and lymphocyte infiltrates in the lamina propria (Fig. 2). Abdominal computed tomography showed diffuse segmental wall thickening together with hyperemia at the rectum and luminal dilatation upstream (Fig. 3).
To treat the proctitis, ciprofloxacin (1,000 mg/day) and metronidazole (1,500 mg/day) were administered. Oral administration of corticosteroids (prednisolone, 10 mg twice daily) was added because symptoms did not improve after one week. After another week, the symptoms improved. We continued loperamide treatment and the patient was transferred to her local hospital for further care. After four weeks, she visited the outpatient gastroenterology clinic and no longer complained of watery diarrhea or abdominal pains. However, the follow-up colonoscopy showed a serpentine-shaped scar, presumably from the large ulcer, at the rectum 5 cm to 7 cm away from the anal dentate line (Fig. 1C, D). Laboratory testing revealed leukocytes of 5,970/mm3, hemoglobin 12.9 g/dL, platelet count 208,000/mm3, and C-reactive protein 0.01 mg/dL.
Discussion
Bisacodyl is a stimulating laxative that has been used widely since 1952. In patients with chronic constipation, colonic transit time and peristaltic movement are delayed and weakened. Bisacodyl acts directly on the colon to increase colon motility [345]. Compared with controls, patients taking bisacodyl demonstrated 23%–31% reduction in colonic transit time and a consequent increase in the water content of the stool [345]. In several studies [345], bisacodyl improved bowel function and constipation symptoms, thereby improving the patient's quality of life. In general, oral bisacodyl is able to reach the intestine through the stomach and small intestine and has a direct effect on the colon. The effect of bisacodyl is evident 6–12 hours after oral intake [345].
The effects of bisacodyl can include abdominal pain, diarrhea, and enteritis, and occasional nausea and headache have been reported [456]. Bisacodyl has been reported to damage the rectal mucosa when taken in the form of suppositories [6789]. Thirty minutes after taking the medication, pathology findings include reduced coloration of cytoplasm and nucleoplasm with loss of epithelium, which is caused by a reduction in hematoxylin and eosin-positive phagocytosis. After 3 hours, chemical damage begins to appear that is indicated by deposition of exudates within the lumen, epithelium, and lamina propria. Neutrophil infiltration is observed 24–30 hours after taking the medication. These findings may be confused with mild acute colitis [679]. The mechanism of bisacodyl-induced damage can be postulated based on studies in rats [10], which showed that in general, the colonic lumen has a lower osmotic pressure than the surrounding blood vessels. Accordingly, water diffuses through the aquaporin3 channels into the blood vessel from the colonic lumen. After rats were given bisacodyl, a decrease in the expression of aquaporin 3 was observed in the epithelial cells in the colon. Thus, water molecules remained within the bowel lumen rather than transferring through the aquaporin channel into the vascular lumen. The consequent increase in colonic volume induced direct physical damage to the mucous membrane of the colon [10]. In addition, bisacodyl induced an increase in the colorectal expression of inflammatory molecules such as tumor necrosis factor-α, cyclooxygenase-2, interleukin (IL)-1β and IL-6 in epithelial cells. It is likely that these mechanisms will also operate in the human body, with similar effects [10]. It has also been reported that there is damage to intestinal mucosa after taking oral bisacodyl: Fjani [11] reported the occurrence of ischemic colitis in four patients after they took oral bisacodyl for chronic constipation. All patients subsequently complained of sudden abdominal pain, diarrhea, and bloody stools for several days. Cessation of the oral bisacodyl and the commencement of fluid therapy with appropriate antibiotics alleviated the ischemic colitis-related symptoms and the patients were discharged. Endoscopy showed edema and ulceration of the intestinal mucosa in two patients and the other two patients demonstrated mucosal lesions, mostly in the descending colon and splenic flexures. The histology showed edema, bleeding from the edematous lamina propria, and an increase in neutrophils.
When taking bisacodyl, colonic motility and luminal pressures are increased, which causes a decrease in the blood flow into the colon, resulting in ischemic colitis [11]. We believe that damage to the intestinal mucosa may occur by this mechanism. In our patient, severe proctitis with rectal ulceration occurred seven days after commencing oral bisacodyl. Antibiotics were administered for two weeks, taking into account the possibility of C. difficile colitis or antibiotic-associated diarrhea. However, stool toxin tests and endoscopic findings were negative for C. difficile colitis, and severe diarrhea persisted even after the cessation of antibiotics. There has been no previous report regarding oral bisacodyl-induced colon ulceration, and because of the patient's chronic constipation, the possibility of isolated rectal ulcer syndrome cannot be excluded. The diagnosis of isolated rectal ulcer syndrome can be made in patients with chronically abnormal bowel habits combined with consistent endoscopic and pathologic findings [1213]. Constipation, bowel movements, tenesmus, abdominal pain, perineal pain, and anal bleeding during bowel movements are the manifestations of isolated rectal ulcer syndrome [1213]. In these patients, colonoscopy may demonstrate several ulcers, primarily in the anterior wall of the rectum 3 cm to 10 cm from the anal verge, and varying in size from 0.5 cm to 4 cm. However, the syndrome may appear as just a congestive change in the rectal mucosa [121314]. Typical pathology findings are a diffuse collagen deposition in the lamina propria and mucosal thickening of the muscle because of the extension of the muscle fibers. In addition, surface erosion and inflammation with mild epithelial dysplasia can be observed [121314]. In our patient, the pathology findings differed from those of isolated rectal ulcer syndrome in that there was no thickening of the lamina propria or smooth muscle fiber hypertrophy. Because there were depositions of neutrophils at the ulceration, damage caused by the oral bisacodyl cannot be excluded; however, it is also possible that severe proctitis might have caused the ulcerations and deposition of neutrophils.
In this case, we can consider bisacodyl induced severe rectal ulcer with proctitis as well as isolated rectal ulcer syndrome. But pathologic findings did not match exactly the common features of isolated rectal ulcer syndrome. So, bisacodyl induced severe rectal ulcer with proctitis cannot be excluded. And based on this case, more research on bisacodyl and rectal ulcer is needed.
There has been no previous report of oral bisacodyl causing severe proctitis and subsequent rectal ulceration. Although the medication is in an oral form, persistent usage may increase the drug concentration in the colonic lumen, which raises the possibility of severe proctitis and subsequent ulcerations in the rectum or even ischemic colitis. Bisacodyl is a relatively commonly used and safe drug. However, in the case of elderly or immobile patients it is recommended that the drug should be administered with care and excessive doses be avoided.


 XML Download
XML Download