

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Ectopic pregnancy is a very common diagnosis (2% of pregnancies) and implantation location varies. About 97% of ectopic pregnancies are implanted within the fallopian tube, and ectopic implantation can occur in other pelvic and abdominal locations [1]. Although very rarely reported, non-tubal ectopic pregnancies might lead to significant diagnostic challenge and morbidity. We report the first case of subserosal myoma ectopic pregnancy, confirmed by laparoscopy and biopsy result.
Case
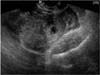
The patient was a 34-year-old, gravida 2 para 1 woman. Her last childbirth was 4 years ago. At admission, the patient was complaining moderate lower abdominal pain. Her last menstrual period was 7 weeks ago and urinary pregnancy test was positive. Her initial blood pressure was 110/80 mmHg, pulse was 72 beats per minute and she was afebrile. The patient's abdomen was soft with lower abdominal tenderness. Trans-vaginal sonography revealed an empty uterine endometrium with 2.35×2.28 cm sized hypoechoic cystic shadow adjacent to the right adnexa (Fig. 1). The anterior cul-de-sac fluid collection was 4.03 cm suggesting hemoperitoneum. Measure of β-hCG was 11,941.1 at presentation.
Initial vital sign was stable, but the patient complained of aggravating pain with notable abdominal distension. Emergency laparoscopy was arranged directly. On operation field, about 500 mL blood collection was seen in pelvic cavity. A bleeding point was noted on the subserosal uterine myoma (2×2 cm) between the right upper body of uterus and right ovary (Fig. 2). The whole mass including myoma was ligated with an endoloop and cut with laparoscopic scissors. The specimen was put in endo-pouch and taken out completely. Dilatation and curettage was done for assuring ectopic pregnancy. Pathologic findings confirmed ectopic pregnancy on uterine myoma; several fragments of myomatous nodule, aggregating about 3.0×2.2×1.8 cm and a separate villous like tissue with blood clot, aggregating about 2.5 mL blocked in myomatous nodule and villous like tissue. Tissues from endometrial curettage showed late secretory phase with predecidual change. The patient was followed up with serial β-hCG measures and trans-vaginal ultrasonography. The level of β-hCG was 2,128.4 IU/mL on the second day and 54.5 IU/mL on the 12th day after the operation.
Discussion
Ectopic pregnancy constitutes 2% of total pregnancy. They are commonly seen in women with history of tubal ligation or pelvic inflammatory disease (PID) and in women with intra uterine device (IUD) for contraception. Ectopic pregnancy is also common in women on medication for infertility. Studies have shown that ovulation induction drug, especially with clomiphene citrate, was an independent risk factor of ectopic pregnancy. Techniques applied in the fallopian tubes, such as zygote and gamete intrafallopian transfer (ZIFT and GIFT), also increased the rate of ectopic pregnancies [2].
Ectopic pregnancy is responsible for the main cause of maternal mortality. We should consider ectopic pregnancy in all women with positive pregnancy test accompanied by abdominal pain or vaginal bleeding. Also, we have to take into account of the possibility of ectopic pregnancy in all case of no intrauterine gestational sac in ultrasonography despite the level of β-hCG is already above the discriminatory zone. We cannot be too careful doubting ectopic pregnancy.
Ninety-seven percent of ectopic pregnancies are located in fallopian tube. Therefore, we may find out ectopic product with ultrasound evaluation of adnexa. But, 2% are ovarian, and the remainder are cervical or abdominal. Also, there are increasing numbers of pregnancies reported within the scar left by caesarean sections [3]. As we experienced, uterine myoma can't be an exception of ectopic implantation site.
A mechanism that probably can explain ectopic pregnancy on uterine myoma of subserosal type is an invasion of the aborted G-sac expelled out from the tubal pregnancy. Another possible mechanism could be a secondary implantation of the abdominal ectopic pregnancy to the pedunculated subserosal myoma. In these possible mechanisms, the first step will be a formation of new microscopic tract of myometrium to the subserosal myoma after trauma from previous uterine surgeries such as curettage, cesarean delivery, myomectomy and hysteroscopy [456]. Then aborted ectopic G-sac implantation may occur in uterine myoma. In this case, primary ectopic pregnancy site might be the salpinx seeing that final ruptured point is the subserosal myoma adjacent to the fallopian tube. Although abdominal ectopic pregnancy could happen anywhere in abdominal cavity, uterine myoma is usually consisted with smooth muscle cells with a few superficial vessel distributed on its capsule is not so hard to implant on.
Because of the rarity of subserosal myoma as an implantation site of ectopic pregnancy, it is not easy to suspect on pelvic sonography at first. In addition to that, subserosal myoma extended laterally from the uterus and may be confused with adnexal or fallopian masses [7]. Mapping of the vascular supply to these myoma can help to distinguish them from adnexal or retroperitoneal tumors including ectopic pregnancies [89].
There are no universal treatment guidelines nor preferred treatment consensus for ectopic pregnancy implanted on the subserosal myoma. However, like in tubal pregnancy, if ruptured, surgical treatment is the treatment of choice. The different thing is in this case, salpinx can be preserved safely because myomectomy is enough to control the bleeding source. Because ectopic pregnancy on subserosal myoma is uncommon entity, a high index of suspicion and the use of trans-vaginal Doppler sonography can help early diagnosis. Because, doppler gives information about the location and degree of blood flow in and around pelvic lesions without the need to inject contrast. So, doppler ultrasound imaging can evaluate the mapping and density of blood flow and even provide a quantitative measure of the amount of blood flow in the implantation site [1011]. We should keep in mind that patient's subserosal myoma could be a site of ectopic pregnancy.

 XML Download
XML Download