

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer had the second highest incidence rate among men and women in 2016 (17.1 deaths per 100,000 individuals) and was ranked as the third leading cause of death after lung and liver cancers (35.1 and 20.9 deaths per 100,000 individuals, respectively), showing a continuously increasing trend in mortality rate from 2007 to 2017.[1] Thus far, the cause of colorectal cancer has not been clarified. Nonetheless, >95% of colorectal cancers have been reported to occur in colorectal polyps, and 5% to 10% of the colorectal polyps can progress to colorectal cancer.[2] Furthermore, the “adenoma-carcinoma sequence” is characteristic of the pathogenesis of colorectal cancer.[3] Hence, the identification of risk factors for colorectal polyps, as well as early colorectal cancer prevention and colorectal polyp detection, is important.
Obesity is known to be an important risk factor for colorectal adenoma and colorectal cancer.[4] However, detailed studies have variously reported the effects of obesity on colorectal neoplasms according to different indicators of obesity and subject characteristics. In a study that used body mass index (BMI), the most commonly used indicator of obesity, no difference in adenoma frequency was observed between obese and normal-weight Korean adults.[5] A meta-analysis of studies with 70,000 cases revealed a higher incidence of colorectal cancer among individuals with BMI ≥30 kg/m2 than that among those with normal weight, although no clear difference was noted between men and women.[6] Abdominal obesity, and not BMI, was an independent risk factor for colorectal adenoma development; however, the association between abdominal obesity and colorectal adenomas was observed to be less relevant in older adults aged >60 years, in whom colorectal adenomas were common.[7]
BMI estimates the obesity level based only on weight and without consideration of muscle and fat quantity, and does not correlate with the total fat percentage in the elderly individuals in whom body composition changes with decreased muscle mass and increased fat mass, which could explain why the association between colorectal adenoma and colorectal cancer has been variously reported according to the obesity index.[8] An increase in age leads to sarcopenic obesity, defined as decreased muscle mass accompanied by increased fat mass. Sarcopenic obesity is considered one of the important problems in older individuals and is associated with metabolic syndrome, cardiovascular diseases, frailty, and mortality.[910] As sarcopenic obesity progresses, muscle strength and mass decrease. A longitudinal study reported significant muscle loss in older participants compared with their younger counterparts and showed that the change in muscle mass was positively correlated with the change in muscle strength (e.g., knee extensor and flexor strength).[11] Handgrip strength, widely used for measuring muscle strength, because of cost, availability, ease of use, and its association with leg strength is related with muscle mass and could be one of the indicators of body composition in the elderly.[1213] The present study aimed to investigate the relationship between colorectal adenoma and grip strength in the elderly.
METHODS
1. Participants
The medical records of participants aged ≥65 years who underwent routine health examination at a local university hospital from July 2015 to September 2018 and responded to self-reported questionnaires were reviewed. Health-screening procedures included physical measurements, laboratory tests, and colonoscopy. Participants aged ≥65 years who were diagnosed with colorectal cancer during the study period (n=1), had a history of any cancer, including colorectal cancer (n=11), or were unable to complete the study because of poor bowel preparation or failure to undergo cecal intubation (n=3) were excluded from the analysis. Finally, 262 participants were eligible after exclusion.
This study was approved by an independent Institutional Review Board (Approval no. 2019-02-012) and was performed in accordance with the principles expressed in the Declaration of Helsinki.
2. Measurement of grip strength
There is no standardized method to measure grip strength; in this study grip strength was measured, in accordance with the method described in many epidemiologic studies, as follows.[14] While sitting on a chair, participants held a dynamometer (Jamar 5030J1; Sammons Preston, Bolingbrook, IL, USA) with their elbow flexed and forearm parallel to the floor and were encouraged to squeeze the apparatus as hard as possible. Grip strength (in kilograms) was alternately measured twice for each hand using the dynamometer. The better numerical value for the dominant hand was used for statistical analysis.
3. Colonoscopy
Experienced board-certified endoscopists performed colonoscopy using a videoscope (CF-Q260AI or CF-Q260AL; Olympus, Tokyo, Japan). Bowel preparations were carried out using a low-volume (2 L) polyethylene glycol solution with 20 g ascorbic acid (Coolprep; Taejoon Pharmaceutical, Seoul, Korea) or sodium picosulfate with magnesium citrate (Picosolution; Pharmbio Korea, Seoul, Korea). The entire colon (i.e., from the rectum to the cecum) was examined, and all the visualized lesions were biopsied and histopathologically assessed by experienced pathologists.
The location, size, number, and colonoscopic appearance of colorectal adenomas were recorded. Hyperplastic polyps were not regarded as neoplastic lesions, and sessile serrated adenoma or traditional serrated adenoma was regarded as colorectal adenoma. The size of each adenoma was estimated using open-biopsy forceps and was categorized as either <7 or ≥7 mm, with the largest adenoma size used in the event of multiple adenomas. The location of adenomas was classified as proximal (including the cecum, ascending colon, or transverse colon) and distal (including the splenic flexure, descending colon, sigmoid colon, or rectum). Histologically confirmed colorectal adenomas were categorized as tubular or tubulovillous and were classified into low-grade and high-grade adenomas, according to the degree of dysplasia. When multiple adenomas were detected, they were prioritized according to the severity of the pathologic findings.
4. Covariates
Participants underwent anthropometric evaluation, including height and weight. Body composition, including muscle mass and percentage of fat, was measured using a bioelectrical impedance analyzer (BIA; Inbody 720; Biospace Co., Seoul, Korea). Blood pressure was measured using an automatic digital BP monitor FT-700R (Jawon Medical Co., Seoul, Korea). Comorbidities, including hypertension and diabetes, and current smoking status were checked by using self-reported questionnaires. Alcohol consumption was defined as alcohol intake more than 2 or 3 times a week, and regular exercise was defined as exercise for more than three times in a week.
5. Statistical analysis
Participants were classified according to sex and presence or absence of adenoma. Continuous variables were analyzed using t-test for the comparison of basic demographic characteristics and were expressed as mean±standard deviation. The χ2 test was used for categorical variables, which were presented as N (%). Subsequently, the characteristics of adenomas in participants with adenoma were analyzed. Multiple linear regression analysis was conducted to estimate the crude and adjusted strength of association between grip strength and number of colorectal adenomas. Outcomes were considered statistically significant if P-values were <0.05. All statistical analyses were performed using IBM SPSS version 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
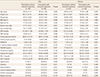
Of the 262 participants included, 144 (55.0%) were men, whereas 118 (45%) were women. The mean age of the men was 69.04 years, irrespective of the presence or absence of adenomas; in contrast, the mean age of the women with adenoma was 70.33 years, which was higher than that of women without adenoma. No difference in obesity, as assessed using BMI, was observed between men and women irrespective of colorectal adenoma. Similarly, body fat percentage and muscle mass, which were estimated by a BIA, showed no statistically significant differences. However, the grip strength in women with colorectal adenomas was significantly different than that in women without adenomas. A similar trend was observed in men, albeit without statistical significance. Furthermore, no differences in insulin resistance, as evaluated using homeostasis model assessment of insulin resistance (HOMA-IR), and comorbidities in men and women were observed between the adenoma and control groups. Lifestyle factors, such as smoking, alcohol consumption, and regular exercise, were not different among participants regardless of sex and the presence or absence of adenomas (Table 1).
The difference in grip strength in relation to the characteristics of adenomas was analyzed in men and women with adenomas (Table 2). The grip strength of men and women with ≥5 adenomas was significantly lower than that of men and women with <5 adenomas. Among men, participants with large adenomas (≥7 mm) had lower grip strength than those with small adenomas. Nonetheless, grip strength showed no relation to dysplasia, pathophysiology, and the location of adenomas in both men and women.
The relationship between grip strength and number of adenomas was analyzed by controlling variables that could affect grip strength and adenomas (Table 3). After adjustment for age, BMI, smoking status, alcohol consumption, and exercise, grip strength was shown to be significantly related to the number of adenomas in both men and women (Model 2). The relationship between grip strength and number of adenomas remained statistically significant after adjustment for insulin resistance evaluated by HOMA-IR and medical history of hypertension and diabetes mellitus (Model 3).
DISCUSSION
In this study, we analyzed whether grip strength, which can be easily assessed in the clinic, is related to colorectal adenoma, a precursor to colorectal cancer. The results of our study indicated that the number of colorectal adenomas was significantly related to a reduction in grip strength, and that grip strength was associated with the size of adenomas in men.
Thus far, few studies have confirmed the association between body composition and colorectal adenoma or cancer. One study, which enrolled adults aged >18 years who underwent medical examination, reported the association between the risk of colorectal neoplasms and skeletal muscle mass, as measured using a BIA.[15] In that study, even after correction for risk factors of colorectal neoplasms such as family history, the negative correlation between muscle mass quartile and the risk for developing colorectal neoplasms remained significant, and muscle mass was observed to be related to advanced colorectal neoplasms in men. A previous study measured muscle mass using BIA in men and women aged ≥40 years and <90% of the standard skeletal muscle mass, and found that participants belonging to the sarcopenia group more frequently had advanced adenomas (adenomas ≥10 mm in diameter, adenomas containing >25% of villous component, and/or high-grade dysplasia or serrated adenoma >10 mm in size).[16] In another study in which muscle mass measured by BIA in adults aged ≥50 years was corrected by weight, and sarcopenia was categorized into classes I and II according to severity, class I sarcopenia increased the risk for developing advanced colorectal neoplasia (adenoma >1 cm in size, any adenoma containing a villous component, high-grade dysplasia, or invasive colorectal cancer) by 1.14 and 1.5 times compared to class II sarcopenia.[17]
The findings of the abovementioned studies suggest that the pathophysiology of muscle loss is considerably similar to that of colonic neoplasms. Increased body weight owing to reduced physical activity, increased production of pro-inflammatory cytokines (interleukin-6 [IL-6], tumor necrosis factor-α [TNF-α]), and decreased level of insulin-like growth factor 1 (IGF-1) are among the major causes of reduced muscle mass and quality in the elderly.[18] Both adipocytes and immune cells (e.g., macrophages) are present in adipose tissues, which secrete various inflammatory substances. Consequently, inflammatory factors, such as C-reactive protein, IL-6, and TNF-α are increased in obese patients. These substances increase muscle catabolism, decrease the amount of muscles, cause malignant tumors in the gastrointestinal tract, and can become risk factors for both colorectal cancer and adenoma.[1019] Like colorectal adenoma, many other gastrointestinal diseases, such as inflammatory bowel disease and celiac disease are linked with osteoporosis, which is closely linked with muscle loss owing to chronic inflammation.[2021] The reduction in muscle mass that occurs during the aging process leads to a decrease in insulin-responsive tissues, resulting in insulin resistance. Furthermore, insulin and IGF-1 are increased in obese patients; they directly inhibit apoptosis and promote cell division, thereby increasing the incidence of colorectal cancer.[22]
Despite the probable link between muscle mass and colorectal neoplasms, several different diagnostic criteria for muscle mass assessment exist. The use of BIA is a relatively easy and rapid method for measuring muscle mass. Nevertheless, magnetic resonance imaging and computed tomography are considered the gold standard for the measurement of muscle mass. Besides, dual-energy X-ray absorptiometry is recognized to be more relatively accurate, but the use of these tools for measurement in the clinic is not easy.[23] Because muscle mass is affected by different body compositions, the evaluation of muscle mass should consider height, weight, and BMI, and the consensus report by the Asian Working Group for Sarcopenia recommends the use of height-adjusted muscle mass indices.[24] However, which indicators suitably reflect health outcomes remains controversial, and various cutoff values have been suggested.[25] Moreover, contrary to predictions, Korean women tend to maintain muscle despite the aging process.[26] Interpretation of the muscle mass of elderly women is difficult, as the index indicates minimal muscle loss.[27] In comparison, measurement of grip strength can be easily and rapidly performed in the clinic and is not difficult to repeat. Various cutoff values for decreased grip strength have been reported, but the difference is not significant compared to the difference in the muscle mass indices. The consensus report by the Asian Working Group for Sarcopenia recommends <26 kg for men and <18 kg for women.[24] In addition, measurement of grip strength is advantageous in that the elderly can intuitively evaluate their condition based on the amount of muscle and can frequently confirm changes attributable to exercise and diet, thereby promoting education and lifestyle changes; furthermore, grip strength is easy to monitor and observe for clinicians.
The present study is the first report on the relationship between muscle strength and colorectal adenomas. In this study, only participants aged ≥65 years in whom the incidence of colorectal adenomas was relatively high were analyzed. The use of the Jamar grip gauge, which is widely utilized for the measurement of grip strength, was also a study strength.[28] Nevertheless, this study has some limitations. It was difficult to elucidate the cause-effect relationship between decreased grip strength and adenoma occurrence with a cross-sectional design. Moreover, selection bias might have occurred, as this study analyzed the health examination data of numerous individuals who were interested in their health and underwent regular checkups. In addition, other risk factors for colorectal cancer and colorectal adenoma, including family history of colorectal cancer and meat consumption, were not examexamined. This study was conducted in one center in Korea. The prevalence of colorectal cancer, dietary habits, and environmental influences differ among different races, so the race of the participants must be considered when interpreting the results. Despite these limitations, understanding the changes in body composition in the elderly and assessing these in detail to clarify their association with health outcomes are valuable. Future studies evaluating health outcome risk according to changes in the body composition of the elderly are required.


 XML Download
XML Download