

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sufficient physical activity is protective against cardiovascular/metabolic complications and lower bone mineral density (BMD) during adolescence.[12] Especially among girls, greater BMD is important due to high prevalence of osteoporosis among older women.[3] Osteoporosis is a public health problem that affects the bone density (degrading the bone structure), leading to a higher risk of fractures.[34] Previous studies have shown that higher physical activity during adolescence is associated with higher BMD during adulthood.[56]
Sport is one of the main physical activities practiced by adolescents. In this sense, the participation in weight bearing sports during adolescence improve the BMD gains and prevent possible future adverse events associated with low BMD.[7] It is widely disseminated by literature that adolescents who participate on land or gravity sports as basketball, track and field or soccer, present relevant gains on total body BMD compared with other non-weight bearing or hypogravity sports.[89101112] A cross-sectional study proposed by Proctor et al.[13] showed that gymnasts presented higher BMD than their control pairs for total body, lumbar spine and right femur.
Moreover, BMD accrual seems an outcome dependent of the sport chosen to be engaged in [1114] being both amount and bone sites where the accrual happens variables affected by sport particularities. Aspects such as running, jumping, changing direction and ball displacement can directly influence this. On the other hand, weekly training load, soil and biomechanics of acrobatic movements and strength of artistic gymnastics (AGs) may present significant differences in BMD.
AGs promotes large mechanical impacts in the execution of its elements (e.g., jumps and acrobatics), specifically, AGs composed of 4 devices: floor, vault (jump on the table), balance beam, and uneven bars. Each device imposes specific mechanical stress requiring strength, balance, flexibility, agility, and muscular power, demonstrating great osteogenic potential.[1314151617] In addition, biological maturation is an important factor that can impact on BMD as well as other tissues during adolescence,[1819] but sometimes not accounted in studies assessing the impact of sports participation on bone outcomes.
Brazil held the Olympic Games in 2016 and, since then, AGs has become more popular in the county, raising doubts of the population about its impact in different health aspects in early life, mainly growth. Although, sports science has advanced in many aspects trying to understand how physical exercise and bone health interact each other during childhood and adolescence, many aspects still unclear, such as the impact of AGs on markers of bone formation and geometrical properties (instead the widely used 2-dimensional BMD).
Thus, our objective was to compare bone density accrual and markers of bone geometry formation, on female adolescents between AGs and control group. We hypothesize, that AG will present higher gains in BMD than its control pairs after the follow-up of 12 months.
METHODS
1. Sample
The Analysis of Behaviors of Children During Growth (ABCD) Growth Study is a longitudinal study which began in 2017. The main aim of this cohort study includes identification of the impact of behavioral variables (e.g., diet, sports participation, sedentary behavior, and sleep quality) on economic and health outcomes (health care costs, metabolic outcomes, intima-media thickness, and bone parameters) among Brazilian adolescents with ages ranging from 10 to 18 years. More details about sampling process are presented elsewhere.[20] Briefly, researchers contacted adolescents in eleven schools and sport clubs spread out in the metropolitan area of Presidente Prudente, a middle-sized city in the west part of the São Paulo state. The sample size calculation was constructed considering a relation between muscle mass and bone mineral content of r=0.84 between adolescent gymnasts,[21] 80% power and 5% error-α. The minimum sample size was estimated in 10 female adolescents in each group (n=20, considering AGs [n=10] and control [n=10]).
Initially, coaches and principals were contacted and they gave the authorization to talk with the students/athletes about the aims of the ABCD Growth Study. The following inclusion criteria were adopted: age ranging from 11 to 18 years, no previously diagnosed disease that could affect daily physical activity, no regular medicine use, having completed the consent form signed by parents/legal guardians and if athlete, at least one year of training experience; if schoolchildren, at least 1 year without practicing any organized sport. All the procedures were previously approved by the ethical committee of São Paulo State University, Campus of Presidente Prudente, State of Sao Paulo, Brazil (Approval no. CAAE: 57585416.4.0000.5402).
2. Inclusion criteria
The inclusion criteria adopted were as follow: (1) The chronologic age between 11 and 17 years old; (2) at least previous 12 months sports participation (gymnastics); (3) non-engagement in organized sports during the last 12 months (non-sports group); (4) no medicine use that may affect the bone metabolism) signed the consent form by parents or tutors.
3. AGs and control group
The baseline measures of the ABCD Growth Study accounted 285 adolescents. In this specific manuscript, only female adolescents engaged in AGs (n=10; age range, 11.8–15.6 years) and controls (n=10) were considered and matched by chronological age P=0.462 and age high peak velocity P=0.473. Gymnasts were involved in championships at state level. After 12 months of follow-up, nine girls in AG group maintained the sports participation, while one dropped the sport after 3 months of baseline measures. In the follow-up measures, researchers successfully contacted this dropout girl and thus this girl has been maintained in all statistical analysis. Among controls, during 12 months follow-up none of those adolescents started any organized sport.
Coaches provided data about gymnasts. At baseline, the previous time of engagement was 58.9 months (95% confidence interval [CI], 34.9–82.8; with minimum 15 months), number of days/week training of 3 days (95% CI, 2.4–3.5; range, 2–5 days), daily training time of 207 min (95% CI, 179.3–234.6; minimum of 150 min) and training volume of 615 min (95% CI, 500.4–729.5; minimum 360 min).
4. Weekly training load
The athletes reported the intensity (according to the rating of perceived exertion) and volume of evert practice session during a week of training (considering the days trained).[22] The training load of each day was calculated multiplying the rating (reported after 30 min of the end of the training) [23] by the volume (total of the day). The weekly training was estimated by the sum of every day.
5. Bone parameters
BMD (expressed as g/cm2) was estimated using a dual energy X-ray absorptiometry (DXA) device (Lunar DPX-NT; GE Healthcare, Little Chalfont, Buckinghamshire, UK) with GE Medical System Lunar software (version 4.7). Every morning before the measurements, following the manufacturer's recommendations, a previously trained researcher assessed the calibration scores of the DXA device. The coefficient of variation of the equipment is 0.66%. A whole-body scan was performed with the adolescents in a supine position, wearing light clothing, barefoot, and without any metal object on the body. In terms of bone outcomes, BMD was measured in the lower limbs, upper limbs, spine, and whole body in both moments of the study (baseline and 12-months follow-up). Additionally, just in the follow-up moment of the study, the participants were positioned to also measure the BMD (neck, trochanter, ward's triangle, shaft, and whole femur) and geometrical parameters (cross-sectional area and cross-sectional moment of inertia) of the femur. In terms of bone formation marker, just in the follow-up moment of the study, osteocalcin levels (expressed in ng/mL) were estimated by a private clinical laboratory (in the morning after 12 hr fasting).
The values of lean soft tissue (LST; expressed as kg) and fat mass (expressed as kg) were also estimated using DXA.
6. Somatic maturation
Body weight was measured on a digital reading scale (Filizola PL 200; Filizzola Ltd., São Paulo, Brazil), with a precision of 0.1 kg, while stature and setting-height were determined using a stadiometer (Sanny, Professional model; Sanny®, São Paulo, Brazil) with a precision of 0.1 cm, according to procedures described in the literature.[24] Age at peak of height velocity were calculated using these anthropometric data.[25]
7. Statistical analyses
Descriptive statistics was composed of mean, standard deviation and 95% CIs. The Student t-test for independent samples compared mean values between the gymnasts and control girls, while analysis of covariance (ANCOVA) compared the same mean values between gymnasts and control girls, adjusted by confounders. For comparisons of variables with non-parametric distribution, was used the Mann-Whitney's test. Pearson's correlation (r) was used to analyze the relationship between numerical variables. All statistical procedures were processed in the statistical software BioStat 5.0 (Instituto Mamirauá, Tefé, Brazil) and statistical significance (P-value) was set at <0.05.
RESULTS
Baseline characteristics of the sample are presented in Table 1, in which gymnastics athletes presented significantly lower body fatness compared to their control peers (P=0.001). All other variables were similar between both groups.
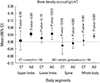
In terms of bone parameters, femur aspects were improved in the group composed of gymnasts, in this case 19% (P=0.009) higher on wards' triangle, 14% (P=0.047) on trochanter and 10% in the overall bone (P=0.046) than control girls. Geometrical parameters and osteocalcin levels were similar in both groups. For bone density, AG group showed significant increase in upper limbs, lower limbs and whole body while control group showed insignificant increase. In the case of spine, the bone density of both groups were decreased but not statistically significant (Fig. 1). There was no significant difference in direct comparison of the change amount between 2 groups (Table 2).
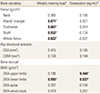
In this sample composed of female adolescents, osteocalcin levels were positively related to bone gains over 12-months follow-up in upper and lower limbs, in which osteocalcin explained 19.7% (r=0.444, r-squared=0.197) and 28.8% (r=0.537, r-squared=0.288) of the bone gains on upper and lower limbs, respectively (Table 3). Similarly, weekly training load (n=10) explained 30.8% (r=0.555, r-squared=0.308) of all bone gains on lower limbs, while weekly training load also was related to higher density on parts of femur (Wards' triangle, trochanter, shaft, and the entire femur). Osteocalcin level and training load positively related to each other (r=0.511, P=0.021).
In terms of femur parameters, in the multivariate models, there was significant difference between controls and gymnasts in wards' triangle (P=0.045) and whole femur (P=0.047) (Table 4). Besides that, the magnitude of the variance explained by gymnastics on all variables was high (neck [15.9%], Wards' triangle [22.8%], trochanter [18.6%], shaft [17.7%], and whole femur [22.5%]). In all models, LST on lower limb constituted the most relevant covariate.
DISCUSSION
The present study aimed to investigate the impact of the engagement in AG on bone parameters in female adolescents after 12 months follow-up.
In the past, many fears were raised about negative impacts on human growth attributed to gymnastics, but the current literature offers support to the promotion of gymnastics as a sports linked to health benefits.[26] In fact, gymnasts present a well characteristic shape which reinforces ideas of natural selection into the modality, in which individuals with a genetic predisposition, such as short stature, tend to stand out in the sport.[2728] Considering the biomechanics and rich variability of movements, individuals with a small stature and lower body mass present advantages over taller and heavier individuals. Therefore, physical characteristics observed in gymnasts seem affected by natural selection, instead harmful impacts on physical growth.[29]
In this longitudinal study, the gymnasts presented higher BMD after 12 months in the ward's triangle and whole femur, as well as, adolescents engaged in AG have significant bone accrual at upper limbs, lower limbs and whole body, while control group have no significant bone improvement. Female AG involves 4 different apparatus (the vault, uneven bars, balance beam, and floor exercise) [30] and the movements performed during practice may explain our results for BMD among gymnasts. With the exception of the floor exercise, the majority of movements and exercises in the AG are performed by the upper limbs, which at many moments are required to support the athlete's entire body weight. In general, AG movements generate compression, tension, and torsional stress in the bones and thus, elevate recruitment of bone formation cells (osteoblasts) at these specific sites.[3132]
The dynamics of acrobatic movements seems relevant to improve bone density on femur on gymnasts, mainly due to the high ground reaction force generated by these movements. For example, plié is a common movement in AG, which exerts great force on lower limbs. Moreover, after plié, gymnasts usually run in the floor in order to increase force and impulse to perform pre-acrobatic plié, in which gymnasts impose maximum strength on quadriceps to assist her in the subsequent jumps, consisting of predetermined movements (e.g., rolling+flip flac+mortal; minichelli+flic flac+extension back with a twist, jump away+cat).[33] In terms of technic, gymnasts also finish the sequence of movements with a reception plié (spiked), showing that movement was finished generating great impact on the skeleton, mainly on the neck of the femur. All these dynamic of movements generate a musculoskeletal tension, which causes micro bone damages, affecting bone remodeling and subsequent bone strength in the segments directly affected by it, especially femur. On the other hand, even considering all those osteogenic elements observed in AG, it is necessary to recognize that its impacts on bone parameters of pediatric groups still under investigation.[153435]
Among female adolescents, the importance of these findings refers to the fact that femur is widely affected by osteoporosis, accounting for largest number of osteoporotic fractures among elderly people.[3436] Therefore, improvements in femur BMD during adolescence might be crucial to prevent osteoporosis in the future.
Osteocalcin level marker of bone formation was slightly higher among gymnasts when compared to controls and positively related to bone density accrual in our sample. Osteocalcin is related to the synthesis and storage of the mineral matrix [37] and its relationship with bone parameters was not a surprise.[34] The impact of sports participation on osteocalcin and the effect of this relationship on bone formation still under investigation, mainly because sports participation might improve bone aspects through other pathways (e.g., bone compression) than just improvements in osteocalcin levels.
Although this study furthers the knowledge of BMD, it also has limitations, being a reduced the sample one of them, which does not allow us to perform more robust analyses or even adjust it by a greater number of potential confounders (the absence of some relevant covariates also is a limitation). Therefore, our findings should be analyzed with caution and every single inference of them made wisely by coaches and health professionals. The small sample size might be responsible by the absence of significant results, but the use of measures of effect-size gives us a new perspective in terms of how interpret our findings and its implications to the real world.[36] Therefore, our findings should be analyzed with caution and every single inference of them made wisely by coaches and health professionals. The lack of evaluation of other bone health parameters such as intake of calcium and vitamin D prevented further deepening of the subject as well as the analysis of osteocalcin and femur at both moments. Despite the limitations already mentioned, this is one of the first studies to analyze BMD gain during 12 months of follow-up, as well as, to relate osteocalcin levels and training with variables, BMD gains of sitios of the body, hip structure and femur sitios.
CONCLUSIONS
In summary, female gymnasts after 12 months follow-up present higher BMD in wards' triangle and whole femur than control group, besides that, femur density was improved in these gymnasts, mainly due to the weekly training load. Lastly, the female gymnasts have a significant bone accrual (after 12 months) in upper limbs, lower limbs and whole body. However, we emphasize the importance in-depth studies that consider other parameters of bone health and with a larger sample size to obtain more structured results.



 XML Download
XML Download