

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Osteoporosis is a common disease characterized by low bone mass and defects in the microarchitecture of bone tissue, which impair bone strength and lead to an increased risk of osteoporotic fractures.[1] Bone mineral density (BMD), measured by dual energy X-ray absorptiometry (DXA), is often employed to diagnose osteoporosis because bone mass accounts for approximately 70% of bone strength.[1] Osteoporotic fractures are one of the leading causes of significant morbidity and disability among elderly people and place a substantial economic burden on health care systems.[2]
BMD is a highly heritable trait, with a heritability ranging between 0.5 and 0.8.[3] Osteoporotic fracture, as an end-point clinical outcome of osteoporosis, has moderate heritability, of approximately 0.5 to 0.7.[3] Most other risk factors for osteoporotic fractures such as bone quality (bone loss, ultrasound properties, bone turnover markers, and bone geometry), and non-skeletal factors (cognition and neuromuscular functions), are also moderately heritable traits.[4] Over the past 6 years, genome-wide association studies (GWASs) and their meta-analyses, assaying hundreds of thousands of single nucleotide polymorphisms (SNPs) in thousands of individuals, have identified over 60 genes/loci associated with variants in BMD and more than 20 genes/loci associated with the risk of osteoporotic fractures. Most GWAS have reported osteoporosis-related variants in Caucasian populations. It is estimated that by 2050, 52% of all hip fractures will occur in Asia, a projected increase from 1990, when 26% of fractures occurred in Asia.[5] However, there are few studies replicating these variants in East Asian populations. A recent study, the largest GWAS meta-analysis to date in the bone field and the second meta-analysis published by the Genetic Factors of Osteoporosis (GEFOS) consortium—(GEFOS-2)—included 32,961 individuals in the discovery stage and was replicated in 50,933 independent subjects.[6] In the discovery stage, most of the data were obtained from Caucasian populations, except for one study from Hong Kong with a sample size of 800.[6] There are ethnic differences resulting from variations in the underlying linkage disequilibrium (LD) structures and in the allele frequencies between Caucasian and East Asian populations.[7] Because these ethnic differences may also influence the results of association studies, it would be interesting to perform genetic susceptibility studies in East Asian populations.[8] In this study, we investigated the association between osteoporosis-related traits (BMD, osteoporosis, or fracture) and BMD-related variants previously reported at the discovery stage in GEFOS-2, in the Korean population. We also investigated the association between osteoporosis-related traits and the variants identified in the Korean cohort, and replicated these variants in other East Asian ethnic cohorts (Chinese and Japanese).
METHODS
1. Study population
1) Korean sample
The Korean cohort included 1,269 postmenopausal women who visited the Asan Medical Center, Seoul, Korea, and participated in the previous GWASs meta-analyses (GEFOS-2).[6] Inclusion and exclusion criteria were previously described.[9] Menopause was defined as the absence of menstruation for at least 1 year and was confirmed by measuring serum follicle-stimulating hormone levels. Patient information such as smoking history (current smoker), alcohol intake (≥3 units/day), medication, previous medical or surgical diseases, reproductive history, history of fractures and family history of fractures, was obtained using a self-administered questionnaire. We intended to improve the identification of genetic factors affecting fractures; therefore, the following were excluded from this study: women exhibiting premature menopause (<40 years of age) and subjects who had taken drugs that potentially affect bone metabolism (e.g., glucocorticoids, sex hormones, bisphosphonates, or other treatments for osteoporosis) for >3 months or within the previous 12 months. In addition, subjects were excluded from the study if they had a history of any disease potentially affecting bone metabolism, such as type 1 diabetes mellitus, cancer, hyperparathyroidism, thyroid disease, or rheumatoid arthritis. Women with dementia or a history of stroke were also excluded due to concerns related to their limited physical activity. Women were also excluded if they had osteophyte formation above fourth points of the Nathan classification system and/or severe facet joint osteoarthritis in the lumbar spine (LS), as determined by conventional spine radiographs.[10]
We measured areal BMD (g/cm2) in the LS (L1 to L4) and femoral neck (FN) by DXA using a Lunar Expert XL system (GE Lunar, Medison, WI, USA) in 700 women and a Hologic QDR 4500-A system (Hologic Inc., Bedford, MA, USA) in the remaining 569 women. Osteoporosis was defined as the lowest T-score ≤ −2.5 standard deviations (SDs) according to the World Health Organization definition.[11] The precision of the Lunar equipment, presented as variation coefficients (CVs) of measurements, was 0.82% for the LS and 1.10% for the FN. The CVs of the Hologic equipment were 0.85% and 1.08% for the LS and FN, respectively. These values were obtained by scanning between 17 and 25 volunteers who were not part of the study. Each volunteer underwent five separate scans on the same day, getting off the table between examinations. To derive cross-calibration equations between the two systems, BMD values were measured in 109 healthy Korean women (mean age 55±11 years; range, 31-75 years) using the two machines. The cross-calibration equations between the two systems were calculated as follows[12]:
Lateral thoracolumbar radiographs were obtained from all participants to determine morphological vertebral fractures. Assessment of vertebral fractures was in accordance with the recommendations of the Working Group on Vertebral Fractures.[13] A vertebral fracture was quantitatively defined as a >20% reduction in any vertebral height measurement (i.e., anterior, middle, or posterior).[14] Non-vertebral fractures at the major osteoporosis-related locations (i.e., hip, distal radius, proximal humerus, and pelvis) were assessed using a self-administered questionnaire. Fractures, clearly caused by major traumas such as motor vehicle accidents or falls from higher than standing height, were excluded. Thus, only low-trauma fractures after menopause were included. When a subject sustained fractures at multiple sites, all sites were included in the analyses.
All study participants provided written informed consent. This study was approved by the Institutional Review Board of the Asan Medical Center.
2) Chinese cohort
The Chinese cohort for BMD consisted of 1,627 subjects.[15] The subjects were recruited from Midwestern Chinese Han adults living in Xi'an and Changsha cities. The exclusion criteria were comparable to those applied to the Korean subjects.[15] LS and FN BMD was measured using the Hologic 4500W machines (Hologic Inc.). The CV values were approximately 1.01% and 1.33% for the LS and FN, respectively.
The Chinese cohort for fractures consisted of 700 Chinese Han subjects (350 with hip osteoporotic fractures and 350 healthy matched controls).[16] All subjects were northern Chinese Han adults living in the city of Xi'an and its neighboring areas. Affected individuals with low trauma hip fractures were recruited from hospitals affiliated with and clinics associated with Xi'an Jiaotong University. Healthy control subjects were enrolled through local advertisements. They were matched to the cases according to geographical proximity and age. Inclusion and exclusion criteria were described previously.[16]
This study was approved by the ethics committee of Xi'an Jiaotong University, and informed consent was obtained from all subjects.
3) Japanese cohort
Japanese subjects included 768 postmenopausal women (aged ≥60 years) from the Rikagaku Kenkyusho (RIKEN) cohort. They were recruited from the BioBank Japan project (http://biobankjp.org/). LS BMD was measured using the Lunar DPX-L (GE Lunar). The CV values were 0.70%. The presence of vertebral fractures was confirmed by radiological examination and a standardized self-questionnaire. Vertebral fractures were defined by expert physicians participating in the study, according to the criteria of the Japanese Society for Bone and Mineral Research.[17] A vertebral fracture was defined as follows: (1) a ratio of the central vertebral height (CVH) to the anterior vertebral height (AVH) <0.8, or a ratio of CVH to the posterior vertebral height (PVH) <0.8; (2) a ratio of AVH to PVH <0.75; and (3) a crushed vertebra was recorded when its height was reduced by >20% in either AVH, CVH, or PVH compared with the adjacent vertebrae. The control populations were not screened for fracture.
Written informed consents from all study subjects were obtained and procedures were approved by the ethics committees of the Institute of Medical Science of the University of Tokyo and other participating clinical institutions.
2. Genotyping
To find the variants showing the association with osteoporosis-related traits (BMD, osteoporosis, or fracture) in the Korean cohort, we used the genotyping data at the follow-up replication stage of BMD loci from the largest previous GWASs meta-analysis (GEFOS-2).[6] Details of the methods were described in the previous GWASs meta-analyses (GEFOS-2).[6] Briefly, a meta-analysis of GWASs of the BMD of the FN (n=32,961) and the LS (n=31,800) was performed. This included approximately 2.5 million autosomal geno-typed or imputed SNPs from 17 studies involving populations across North America, Europe, East Asia, and Australia. A total of 96 independent SNPs from 87 genomic loci were selected for the follow-up replication stage of BMD loci in the GWAS meta-analysis. The 96 variants included the 82 index SNPs, representing each of the 82 loci reaching P<5×10−6 in the meta-analysis of the 17 GWASs of BMD, 9 SNPs located within the same 2 Mb windows as the 82 loci but independent from the main signal (secondary signals), and the top five most-associated SNPs of the X chromosome (with P<5×10−5). Korean samples were directly genotyped for replications of the 96 selected SNPs at deCODE Genetics (deCODE Genetics/Amgen, Inc., Reykjavik, Iceland). The genotyping was performed on a Centaurus (Nanogen, San Diego, CA, USA) platform. The quality of each Centaurus SNP assay was evaluated by genotyping each assay in the CEU HapMap samples and by comparing the results with the HapMap data. Assays with mismatches >1% were not used, and positive and negative controls were presented on all genotyping plates to ensure correct genotyping. Functional assays meeting all quality criteria could not be performed for the markers rs4727338, rs4869742, rs6959212, rs430727, rs1286083, rs6532023, rs4790881, rs12995369, and rs4792909, and these proxy SNPs—rs7781370, rs4870044, rs1403987, rs87938, rs1286077, rs1471403, rs11657636, rs11690020, and rs7220711—were genotyped instead, respectively. For the SNP rs11048046, a functional assay could not be performed nor was there a known proxy SNP available. Finally, 95 SNPs were genotyped. Genotyped calls were centrally controlled for sample call rate >80%, SNP call rate >90%, P>1×10−4 for deviations from Hardy–Weinberg equilibrium (HWE), and minor allele frequency (MAF)>1%.
The Chinese cohort for BMD and fracture cohorts was genotyped using Matrix Associated Laser Desorption Ionization-Time Of Flight (MALDI-TOF) mass spectrometry on a Sequenom system (Sequenom Inc., San Diego, CA, USA) with iPLEX assay.[18] Primers were designed using MassARRAY Assay Design 3.1 software. Genotyping quality control procedures leading to SNP exclusion were the following: call rate <90%, MAF <0.05 in the total sample and P<0.001 for deviations from HWE in controls. In the Chinese sample for BMD cohorts, 10 (rs7326472, rs17040773, rs9921222, rs730402, rs87938, rs1564981, rs10048146, rs3736228, rs1373004, and rs2016266) of 35 SNPs were genotyped and a further 25 SNPs were imputed using the 1000 Genomes Project. In the Chinese sample for fracture cohorts, 6 (rs7326472, rs17040773, rs730402, rs87938, rs3736228, and rs1373004) of 35 SNPs were genotyped and a further 29 SNPs were imputed using the 1000 Genomes Project. The Japanese cohort was genotyped using the Invader assay, according to the manufacturer's instructions.[19]
3. Selection of risk alleles
To identify risk alleles, all 95 SNPs were tested to determine their independent association with osteoporosis-related traits (low BMD or the presence of osteoporosis or osteoporotic fracture). A risk allele was an allele associated with a decreased BMD, increased risk of osteoporosis, or fracture at vertebral, non-vertebral, and any sites, with marginal significance if the P values were lower than 0.05 but higher than α, significance level of Bonferroni correction for multiple testing (α=0.05/35 SNPs/three genetic models=0.00048).[9]
4. Statistics
All data are presented as means (SD) or as numbers (%). The χ2 test was used to determine whether individual variants were in equilibrium at each locus in the population (HWE). Genotypes were assigned codes of 0, 1, and 2 for the additive model; 0, 1, and 1 for the dominant model; and 0, 0, and 1 for the recessive model. Multivariate linear regression analyses of LS and FN BMD were performed using age, sex (only applicable to Chinese subjects), weight, and height as covariates. Genotype distributions between participants with or without fracture were analyzed using a logistic regression model, controlling for age, sex (only applicable to Chinese subjects), weight, and height. All statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Table 1 shows the baseline characteristics in the study population. Chinese BMD cohorts were younger than the other cohorts were. Non-vertebral fractures in Chinese and Japanese subjects only included hip fractures. Only LS BMD was measured in Japanese subjects.
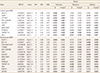
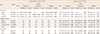
First, we investigated the association between osteoporosis-related traits (BMD, osteoporosis, or fracture) and 95 SNPs in the Korean cohort (Tables 2, 3). A total of 17 SNPs from 17 loci were associated with low BMD (β=−0.008 to −0.174, P=0.001 to 0.048) (Table 2) in Korean subjects. A total of 9 SNPs from 9 loci were associated with osteoporosis (odd ratios [ORs] 1.20-2.20, 95% confidence intervals [CIs] 1.00–4.64, P=0.012–0.049] (Table 3). A total of 6 SNPs from 6 loci were associated with the presence of non-vertebral fractures (ORs 1.40–4.14, 95% CIs 1.00–13.33, P=0.008–0.048) (Table 3). A total of 9 SNPs from 9 loci were associated with the presence of vertebral fractures (ORs 1.33–9.98, 95% CIs 1.02–34.96, P<0.001–0.040) (Table 3). A total of 5 SNPs from 5 loci were associated with the presence of any fracture (ORs 1.28-8.67, 95% CIs 1.00-29.03, P<0.001-0.049) (Table 3). Collectively, 35 out of the 95 SNPs (36.8%) were associated with one or more osteoporosis-related traits in Korean subjects.
Second, we investigated the association between osteoporosis-related traits and 35 variants in the other East Asian ethnic cohorts, the Chinese and Japanese cohorts (Tables 4,5). A total of 12 SNPs from 12 loci were associated with low BMD (β=−0.009 to −0.041, P=0.002–0.049) (Table 4) in Chinese and Japanese subjects. A total of 3 SNPs from 3 loci were associated with hip fractures (ORs 1.26–1.78, 95% CIs 1.02–2.70, P=0.006–0.036) (Table 5). A total of 4 SNPs from 4 loci were associated with the presence vertebral fractures (ORs 1.44–2.10, 95% CIs 1.01–4.27, P=0.019–0.043) (Table 5). A total of 2 SNPs from 2 loci were associated with the presence of any fracture (ORs 1.30–2.37, 95% CIs 1.01–4.99, P=0.020–0.044) (Table 5). Finally, 19 SNPs (54.3%) out of 35 SNPs were associated with one or more osteoporosis-related traits in East Asian ethnic populations.
DISCUSSION
In the present study, 35 out of the 95 SNPs (36.8%), previously identified in largely Caucasian populations, were associated with one or more osteoporosis-related traits in Korean subjects. Furthermore, 19 out of the 35 SNPs (54.3%) were also associated with one or more osteoporosis-related traits in the 4,414 East Asian ethnic populations (Chinese, Japanese, and Korean, combined). Therefore, these 19 SNPs were common variants of osteoporosis-related traits in both Caucasian and East Asian populations.
Among Korean subjects, 35 SNPs from 34 loci were associated with one or more osteoporosis-related traits. Some of these genes are known to play a critical role in several biological pathways influencing osteoporosis and fracture susceptibility. First, some genes including AXIN1, CTNNB1, DKK1, LRP5, WLS, WNT4, WNT5B, and WNT16, participated in the Wnt/β-catenin signaling pathway. Second, SOX9 and SP7 were involved in mesenchymal stem cell differentiation and endochondral ossification. Third, CLCN7 and LRP5 were associated with rare monogenic forms of osteoporosis and/ or high bone mass. Finally, TNFRSF11A (encoding the receptor activator of nuclear factor-kappa B [RANK]) and TNFRSF11B [encoding the osteoprotegerin (OPG)] were involved in the RANK ligand (RANKL)/RANK/OPG pathway. Out of 14 loci which were significantly associated with any type of fracture at Bonferroni-corrected level of significance (P=5×10−4) in the previous GWASs meta-analysis (GEFOS-2), 4 SNPs from 4 loci, including C18orf19/FAM 210A (rs4796995, 18p11.21), DCDC5 (rs163879, 11p14.1), WNT16 (rs3801387, 7q31.31) and WNT4 (rs7521902, 1p36.12), were also associated with fractures.[6]
Of the 64 BMD-related SNPs from 56 loci at genome-wide significance (P<5×10−8) in the largest previous GWASs meta-analysis (GEFOS-2), 29 SNPs (45.3%) from 28 loci were associated with osteoporosis-related traits among Korean subjects.[6] Out of the rest 31 SNPs which did not reach the genome-wide significance in the previous study (GEFOS-2), 6 SNPs (19.4%) were associated with osteoporosis-related traits in Korean, as follows: AKAP11 (rs7326472, 13q14.11), ANAPC1 (rs17040773, 2q13), BCL11A (rs730402, 2p16.1), CYP19A1 (rs2118784, 15q21.2), NAB1 (rs11675051, 2q32.2), and PLVAP (rs7257450, 19p 13.11).[6] The differences in results between the this study in Korean and the discovery stage analysis of the previous study (GEFOS-2) in Caucasian may be explained by ethnic differences, such as differences in allele frequencies and underlying LD structures and by the small sample size of this study (n=1,269).[320] Another possible explanation for the differences in results between this study and the previous study (GEFOS-2) could be the heterogeneity of the study design including differences in the phenotype (osteoporosis, BMD, BMD site, fracture, and fracture type), in the adjusted covariates (age, weight, and height), and in the genetic model differences (additive, dominant, and recessive models). Considering the replication rate of BMD phenotype, 17 (17.7%) of the 96 BMD-related SNPs were associated with BMD in the Korean cohort. Associations of some SNPs in this study were only showed in the recessive models, so heterogeneity of genetic models between this study (additive, dominant, and recessive models) and the previous study (additive model) might be the differences in results.[6]
To compare the replication rate of 95 SNPs in Korean women, we checked the replication rate of the previous Korean study involving 1,586 unrelated Korean women from a population-based cohort.[21] Out of the 717 SNPs, there were 89 SNPs which were included in this study. The replication rate in this study (36.8%; 35 out of 95 SNPs) was comparable to that of a previous study (30.3%; 27 out of 89 SNPs).[21] The differences in replicated SNPs among Korean subjects may be due to the use of different phenotypes between this study (BMD, osteoporosis, or fracture) and the previous study (only BMD). Another possible explanation for the differences in replicated SNPs could be the lack of statistical power due to the small sample size of both this study (n=1,269) and the previous study (n=1,586). The 14 replicated SNPs in both Korean studies were as follows: AKAP11 (rs9533090, 13q14.11), CTNNB1 (rs87938, 3p22.1), DNM3 (rs479336, 1q24.3), FOXL1 (rs10048146, 16q24.1), GALNT3 (rs1346004, 16q24.1), LEKR1 (rs344081, 3q25.31), RPS6KA5 (rs1286077, 14q32.12), TNFRSF11B (rs2062377, 8q24.12), WLS (rs12407028, 1p31.3), WNT16 (rs3801387, 7q31.31), WNT4 (rs7521902, 1p36.12), ZBTB40 (rs6426749, 1p36.12), BCL11A (rs730402, 2p16.1), and PLVAP (rs7257450, 19p13.11). Therefore, these 14 SNPS may represent true osteoporosis-related genetic markers in the Korean population.
Of the 35 SNPs associated with the osteoporosis-related traits in Korean subjects, 19 SNPs (54.3%) were associated with one or more osteoporosis-related traits in the other East Asian ethnic populations (Chinese and Japanese). Therefore, these 19 SNPs, AKAP11 (rs9533090 and rs7326472), ARHGAP1 (rs7932354), AXIN1 (rs9921222), C16orf38 (rs13336428), C17orf53 (rs227584), C18orf19 (rs4796995), CTNNB1 (rs87938), CYLD (rs1564981), CYP19A1 (rs2118784), GALNT3 (rs1346004), KIAA2018 (rs1026364), LRP5 (rs3736228), MPP7 (rs3905706), RPS6KA5 (rs1286077), WLS (rs12407028), WNT16 (rs3801387), WNT4 (rs7521902), and ZBTB40 (rs642674), may represent true osteoporosis-related genetic markers, regardless of ethnicity. Furthermore, WNT16 (rs3801387) may represent true osteoporotic fracture-related genetic markers regardless of ethnicity. The replication failure was also reported in East-Asian populations. Heterogeneity, including different phenotype (measured site of BMD and type of fracture) and other confounding factors (age, sex, weight, and height) among the three East Asian ethnic populations, may have affected the association analyses in our study.[3] Previous genetic studies showed sex and site specificity underlying BMD variation.[6] The proportions of cortical and trabecular bone differ at the different sites (e.g., hip, spine and wrist). Furthermore, each type of fracture has its own unique risk factors.[22] For instance, falls are a major risk factor for hip and wrist fractures; however, they contribute little to the risk of vertebral fractures. Epidemiology data also show that the prevalence of fractures at different sites is different according to age, sex, and ethnicity.[22]
Our study has several limitations. First, the associations of the selected risk alleles were marginally significant [α (significance level of Bonferroni correction for multiple testing <P<0.05; α=0.05/35 SNPs/three genetic models=0.00048). Therefore, there was the possibility of false positive results because multiple tests were performed. In addition, the lower replication rate of the SNPs which did not reach did not reach the genome-wide significance (19.4%) than that of the SNPs at genome-wide significance (45.3%) may suggest that some of 96 SNPs were candidate SNPs with considerable risk of false positivity. However, 35 SNPs were associated at P<5×10−6 in the discovery set of the GWAS and were tested for replication of association here.[6] Second, there were some heterogeneity and other confounding factors among the three East Asian ethnic populations. Although we adjusted for age, sex, weight, and height, these confounding factors may have affected the results of the association analyses. Meta-analyses with less between-sample heterogeneity and other confounding factors, which may increase the power of study, were needed. Third, the design of our study was cross-sectional.
In summary, our results showed the common variants of osteoporosis-related traits in both Caucasian and East Asian populations. The possibility that these SNPs may represent true osteoporosis-related genetic markers should be further investigated.



 XML Download
XML Download