

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stroke is one of the leading causes of disability in the world [1] and has a large impact on patients and their family members [2]. Neurological symptoms after a stroke vary according to the location and extent of the brain lesion, but motor weakness and cognitive impairment are the most frequently reported symptoms [3]. Immediately after a stroke, up to 85% of the survivors experience impairment of the hemiparetic upper extremity [4]. Eighty percent of these patients achieve their best upper extremity function within 3 weeks of stroke onset and 95% achieve it within 9 weeks [4]. However, between 55% and 75% of the stroke survivors have persistent functional limitations of the upper extremity, resulting in dependency for activities of daily living (ADL) [5]. Attention deficits are also commonly observed after stroke. Although the exact frequency is a matter of debate, the prevalence has been estimated to be 46%-92% in the acute phase [6] and 24%-51% at discharge [7,8]. One report suggested that up to 50% of the stroke survivors developed attention deficits that persisted for years after the stroke [9].
Since virtual reality (VR) technologies were first developed, VR-based therapy has been viewed as a promising rehabilitation tool [10]. VR-based therapy uses interactive simulations that are created by computer hardware and software to provide environments that mimic the real, three-dimensional environment, which encourage users to be engaged in activities [11] regardless of their physical disability. Currently, VR technologies in stroke rehabilitation have predominantly targeted motor recovery. A Cochrane review concluded that VR was an effective treatment for recovery of upper extremity motor function and ADL after stroke, when compared to the conventional rehabilitation therapy [12]. Furthermore, Kim et al. [13] demonstrated that VR training combined with computer-based cognitive rehabilitation had a significant effect on visual attention and short-term visuospatial memory in stroke patients with cognitive impairment.
Unfortunately, most VR interventions are hospital-based and have several obstacles to overcome, such as being expensive and bulky, and most of them are dependent on therapist. However, commercial computer gaming equipment uses a wireless controller to interact with the player through a motion detection system and avatar technology (e.g., Wii; Nintendo, Tokyo, Japan), and this has been used as a new style of VR equipment [14]. The commercial gaming is relatively cheap and easy to use, and a few studies have reported that it can promote motor recovery after stroke [14,15,16,17,18].
However, most of the existing trials were pilot studies [2,14,15,18,19] and they only compared commercial computer gaming to recreational therapy [2,14]. There is no study that has compared commercial computer gaming (Wii) with conventional occupational therapy (OT). Also, the existing studies only recruited patients with mild hemiparesis, because the intervention required the patient to grip the remote control [2,14]. In addition, although commercial gaming-based VR therapy is composed of complex activities using visual and auditory stimulation and requires continuous attention, there was no research about cognitive training by commercial gaming.
The aim of this study was to determine whether commercial gaming-based VR therapy was as effective as conventional OT for functional recovery of the hemiparetic upper extremity and attention deficits in subacute stroke patients.
MATERIALS AND METHODS
Participants
Twenty patients who experienced a stroke for the first time within the last 3 months were recruited from the Department of Rehabilitation at Jeju National University Hospital between September 1, 2012 and June 30, 2013. Our protocol was reviewed and approved by the Institutional Review Board of Jeju National University Hospital, and all participants provided written informed consent before the selection procedure.
This was a randomized, single-blind study. Participants were randomly allocated in a 1:1 ratio to the 2 study groups. The randomization schedule was achieved by using a 'sealed envelope' technique. The assessor was blinded whether the participants were in case group or control group.
The study sample comprised of ten males and ten females with a mean age of 64.72±10.6 years. The inclusion criteria were as follows: 1) clinical diagnosis of subacute stroke confirmed by neuroimaging (computed tomography or magnetic resonance imaging), 2) hemiparesis of the upper extremity (upper limb score of the Fugl-Meyer Assessment <50), 3) a manual muscle testing (MMT) grade of more than 2/5 in the hemiparetic shoulder, and 4) ability to follow instructions that involved more than one step. The exclusion criteria were as follows: 1) cognitive dysfunction or aphasia severe enough to preclude task performance, 2) visual impairment or spatial neglect, 3) contracture or deformities in upper extremity, 4) metallic implants in the intracranial space or a pacemaker, and 5) previous history of epilepsy.
Intervention
Participants were randomly assigned to the experimental group (n=10) or the control group (n=10). Participants in the experimental group received commercial gaming-based VR movement therapy using the Wii (Nintendo) for 30 minutes a day. Participants in the control group received conventional OT for 30 minutes a day. Both interventions were delivered five times a week for 4 weeks, and both groups also received conventional rehabilitation therapy except for OT.
To prevent further injury, all participants in the experimental group who had more than grade 2/5 and less than grade 3/5 in MMT of the shoulder wore a shoulder sling during the commercial gaming-based VR movement therapy under the supervision of occupational therapist. The patients in the experimental group who could not grip the remote control used a newly developed forearm orthosis which fixed the remote control onto the hemiparetic forearm with straps (Fig. 1). We use the Wii Sports Resort (Nintendo) program which consists of 12 games. The swordplay, table tennis, and canoe games were used in the current study, as these involve motor function and are of interest to older patients. The swordplay game involved performing flexion, extension, internal and external rotation of the shoulder, and flexion and extension of the elbow. The table tennis and canoe games also required upper extremity motions including internal and external rotation of the shoulder, flexion and extension of the elbow, and pronation and supination of the forearm. All the participants were instructed to play the games with their hemiparetic upper extremity. However, the patients who had motor weakness of proximal upper extremity of less than grade 3 in MMT were allowed to use non-paretic hand to support the hemiparetic side.
Conventional OT was goal-oriented and highly repetitive trainings assisted by occupational therapist. It was composed of stretching and strengthening exercises using full range of motion of the upper extremity, which was a task-oriented therapy for the ADL, fine motor training, and sensory motor recovery. The occupational therapist chose the appropriate tasks for the individual patient and developed them in stages.
Outcome measures
Outcome measurements were evaluated before and at the end of the 4-week intervention in all participants.
Primary outcome measure
The upper limb score in the Fugl-Meyer Assessment (FMA-UL) was used for primary outcome measure to assess the motor function of both upper extremities including the shoulder, elbow, forearm, wrist, and hand. The FMA-UL is widely used for comprehensive clinical examination of arm function, and the maximal score of FMA-UL is 66 points [20].
Secondary outcome measures
The patients were also evaluated of the upper extremity motor functions by manual function test (MFT), box and block test (BBT), and grip strength. The MFT consisted of 8 items as follows: forward and lateral elevation of the arm, touching the occiput and the back with the palm of the hand, grasping, pinching, carrying a cube, and pegboard manipulations. The MFT score ranged from 0 points (severely impaired) to 32 points (full function) [21]. The BBT was used to evaluate gross manual dexterity of the hemiparetic upper extremity. The number of cubes that the participant transferred during 1 minute was counted; a higher number indicated better function [22]. Grip strength of the paretic hand was evaluated using a dynamometer. The participant was seated with the hand resting comfortably on the laps and was instructed to flex the fingers maximally. The procedure was repeated three times and the highest score from the three trials was used for analysis [23].
The Korean version of the Mini-Mental State Examination (K-MMSE) was used to evaluate cognitive function [24]. The visual and auditory continuous performance tests (CPTs) of the computerized neuropsychological test (CNT; MaxMedica Inc., Seoul, Korea) were used to assess attention. Performance on the CPTs was quantified using reaction time and commission errors [25].
The Korean version of the Modified Barthel Index (K-MBI) was used to evaluate ADL function. The K-MBI was a reliable, valid tool for measuring the ADL of patients in Korea [26].
Statistical analysis
The change in each outcome measurement from pre- to post-intervention was evaluated separately in each group using a Wilcoxon signed-rank test. The change in each outcome measurement from pre- to post-intervention was compared between the two groups using a Mann-Whitney test. A p-value of less than 0.05 was considered as significant. Statistical analyses were performed using SPSS for Windows ver. 20 (IBM-SPSS Inc., Armonk, NY, USA).
RESULTS
Baseline characteristics
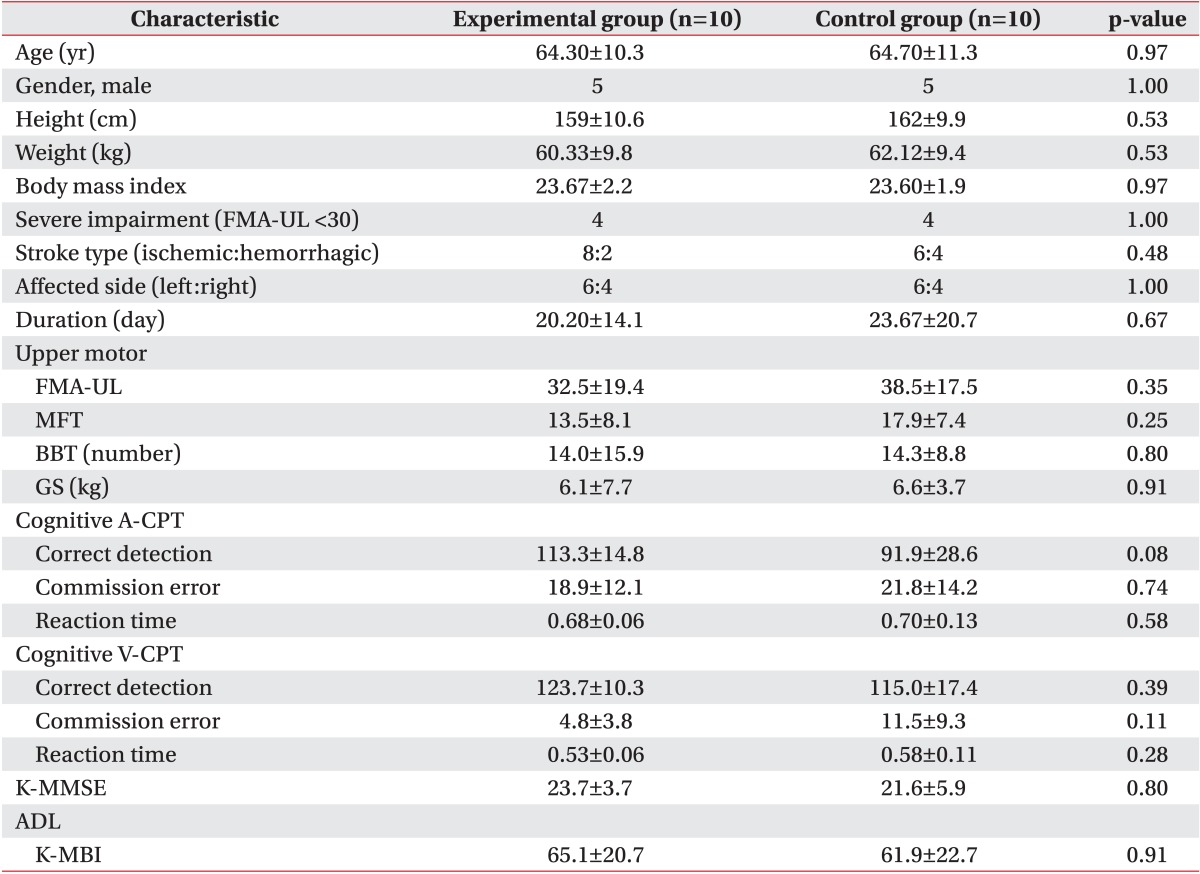
The baseline demographic characteristics of the participants are summarized in Table 1. Demographic characteristics including gender, age, body mass index, stroke type (ischemic or hemorrhagic), affected side (right or left), and the duration from stroke to the first evaluation were not significantly different between the two groups. Twenty-one patients were eligible, but one patient refused to consent. All 20 participants completed both treatments. None of the participants experienced a serious adverse event during the study period.
Hemiparetic upper extremity motor function
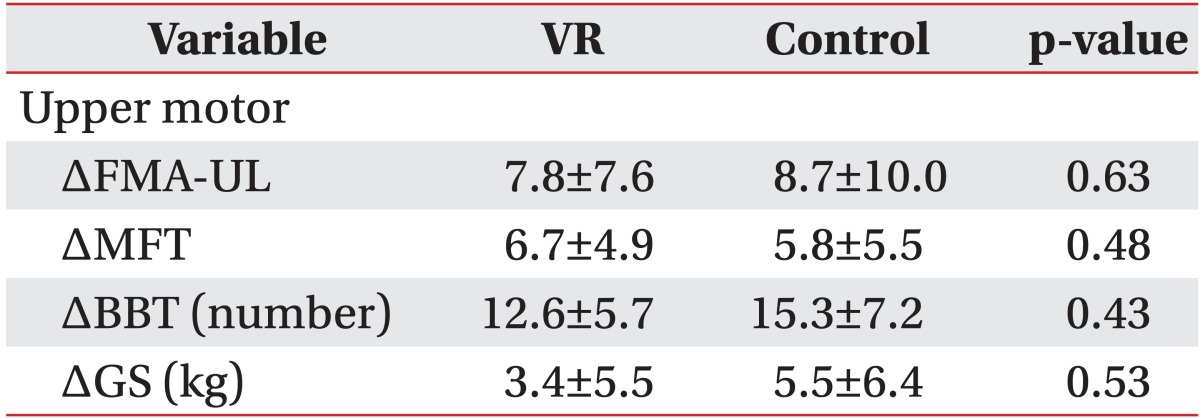
Hemiparetic upper extremity motor function outcomes score are presented in Tables 2 and 3. There were no significant differences between the two groups at baseline (Table 1). FMA-UL, MFT, and BBT scores improved from pre- to post-intervention in both groups. Grip strength of hemiparetic hand improved only in the control group (Table 2). There were no significant differences between the two groups before and after the 4-week intervention (Table 3).
Cognitive function and ADL
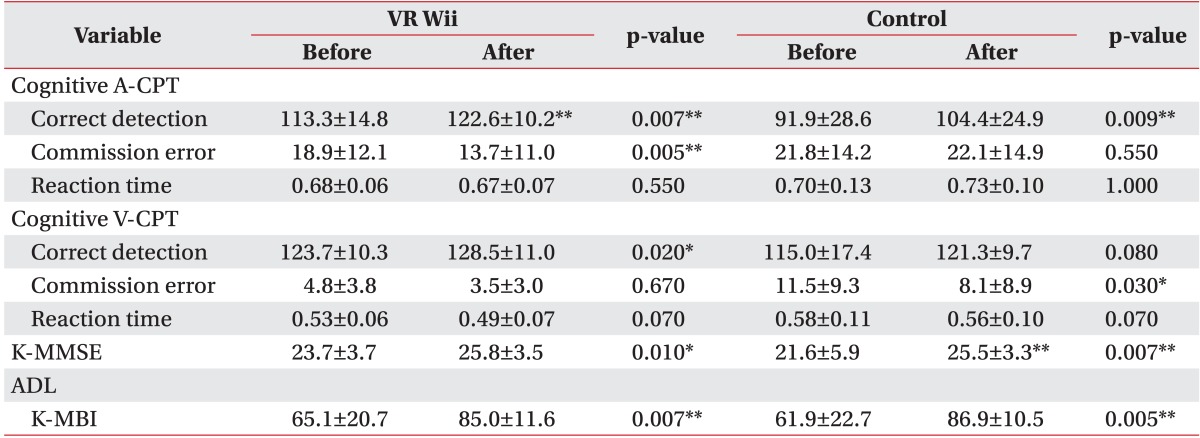
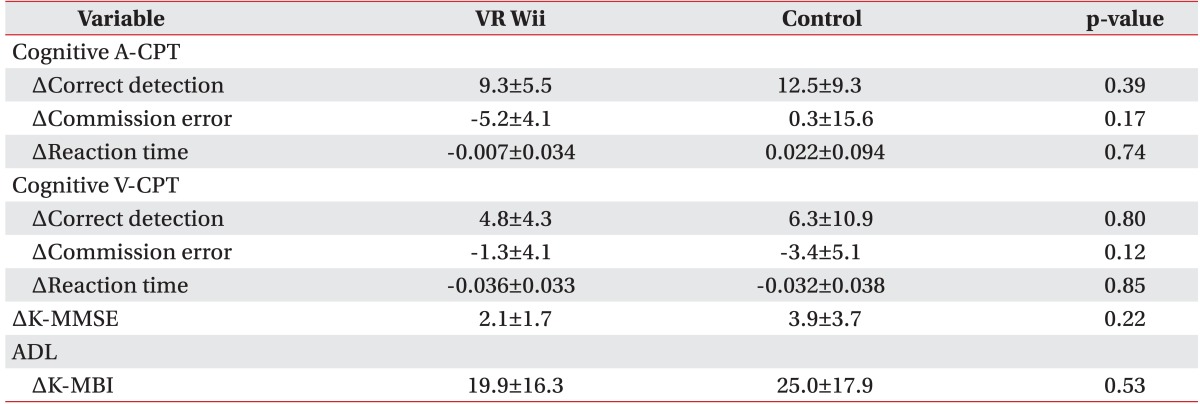
There were no significant differences between the two groups at baseline (Table 1). K-MMSE score, the number of correct detections in the auditory CPT, and K-MBI scores increased from pre- to post-intervention in both groups (Table 4). The number of commissure errors in the auditory CPT and number of correct detections in the visual CPT improved only in the experimental group (Table 4). The K-MMSE, visual and auditory CPT, and K-MBI scores did not reveal any statistical differences between the two groups before or after the 4-week intervention (Table 5).
DISCUSSION
Our results demonstrated that commercial gaming-based VR movement therapy was as effective as conventional OT for the recovery of upper extremity gross motor function and ADL in subacute stoke patients with moderate to severe motor impairment.
Coupar et al. [27] reported that the most significant predictor of upper limb recovery after stroke was the initial severity of motor impairment or function, and the severely hemiplegic patients might develop persistent disability. Therefore, various methods for gaining the best possible improvements in upper extremity function had been studied including bilateral movement therapy, constraint induced movement therapy, functional electrical stimulation, VR, and OT. Although there is no standard protocol for upper extremity therapy after a stroke, the current focus is on high-intensity, task-oriented, repetitive training of the paretic upper extremity [28,29].
Commercial gaming-based VR movement therapy would be an effective alternative to high-intensity, task-oriented, repetitive training after a stroke. However, the use of this therapy had been limited, because it could not be applied to patients who were unable to grip the remote control. We developed a forearm orthosis that could hold the remote control, and it enabled severely hemiparetic patients (FMA-UL <30) to participate in the VR movement therapy in the present study. We evaluated the function of the paretic upper extremity using the FMA-UL, MFT, BBT, and grip strength. The FMA-UL is a valid and reliable scale that is widely being used for comprehensive clinical examination of arm function [30], and we selected this as the primary outcome. The total FMA-UL is 66 points, and the scores between 50 and 65 indicate mild impairments, scores between 30 and 49 indicate moderate impairments, and scores below 30 indicate severe impairments [31,32]. After the 4-week intervention, both groups showed improvement in the score of FMA-UL. Also, both groups showed significant improvements in K-MBI, MFT, and BBT scores; but only the control group showed an improvement in hand grip strength. These results indicated that our VR movement therapy had significant effects on ADL and arm function, but not on hand grip strength. Cochrane review of VR for stroke reported that VR did not show significant differences in grip strength compared to alternative therapy [12,33]. The conclusion of our study is almost consistent with those of others described above, except that grip strength has been improved after the treatment only in control group. The lack of improvement in hand grip strength could be explained by several hypotheses. First, previous studies recruited patients with better functions in BBT and grip strength [14] or in FMA-UL [18], than those of our research. In the present study, the participants with severe hemiparesis who could not grip the remote control used a forearm orthosis to participate in the VR movement therapy. Therefore, they did not perform a hand grip movement during the therapy. Secondly, our VR movement therapy protocol consisted primarily of gross arm motions including shoulder, elbow, and forearm movements, and it did not include strengthening or fine motor training of the paretic hand and complex cognitive tasks.
Although we observed improvements in some CPT parameters, reaction time in the visual and auditory CPTs did not significantly change after the intervention. Therefore, the results showed incoherent findings in both groups; there was no difference in the changes from pre- to post-intervention between the experimental and control groups.
Specific cognitive training program were composed of various complex tasks including attention, memory, learning, and problem solving. Although our participants had to interact with computer-stimulated environment which required continuous attention to achieve higher score, our study did not provide any evidence supporting a sufficient, beneficial effect of commercial gaming-based VR movement therapy on attention.
Conventional OT is usually delivered in a hospital setting over a limited time frame, due to therapist-dependency and economic cost [34]. In contrast, commercial gaming-based VR movement therapy could provide continuous training of the upper limb, and it can be used at home or in a group setting. Commercial gaming was familiar, interesting, and cheaper than other VR methods used in a hospital setting. Additionally, commercial gaming-based VR movement therapy enhanced motivation and interest which in turn increased the patients' compliance [35,36]. It provided interactive stimulation and feedback [11], which is fundamental to motor skill learning [37]. In addition, higher motivation has been associated with better rehabilitation outcomes [35].
A recent systematic review confirmed the effect of VR therapy on upper limb recovery and ADL function after a stroke and highlighted the potential value of commercial VR gaming as a tool for stroke rehabilitation [12]. Our conclusion was consistent with this view. However, much more evidence is needed to establish a standardized protocol that would be targeted at the specific impairment and the ADL of stroke patients.
There were several limitations to our study. Firstly, we were unable to perform subgroup analyses according to the baseline severity of motor impairment, due to the small sample size. Secondly, although we randomly assigned the patients into each group, the study was single-blind and it is possible that patients using the new VR technology were more motivated than patients receiving OT. Thirdly, due to the short duration of treatment, we are unable to conclude on the long-term effect of commercial gaming-based VR movement therapy on upper extremity motor function, cognitive function, or ADL. Fourthly, the commercial gaming programs were too easy and simple to be used as a cognitive training method. Although it used visual and auditory stimulus, specific cognitive virtual reality program might be recommended for a cognitive training. Finally, commercial gaming programs were designed for healthy individuals and the feedbacks were provided based on the movement itself; but the target movements were not necessarily the ideal adaptive responses. As a result, supervision of the caregiver might be necessary in subsequent trials to optimize VR therapy.
Further research involving a larger sample size and long-term for follow-ups should be performed to compare participants according to the baseline severity of upper extremity impairments and to establish a standardized gaming program for post-stroke rehabilitation.
In conclusion, our findings demonstrated that the commercial gaming-based VR movement therapy was as effective as the conventional OT for functional recovery of upper extremity motor function and ADL function. Therefore, we suggest the commercial gaming-based VR movement therapy to be used as an alternative method for self-oriented or home-based occupational rehabilitation therapy for subacute stroke patients.


 XML Download
XML Download