

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Regular physical exercise is an important aspect of a healthy and long life.1 Patients with spinal cord injury (SCI) have a limited ability to exercise or regulate their body weight in their lower extremities because they are restricted to a wheelchair, which can lead to various complications. Prevention, management of complications, and comprehensive rehabilitation therapy are important since respiratory, circulatory, digestive, urinary, and musculoskeletal complications can occur in patients with SCI.2 Physical exercises after SCI can maximize an independent life and enhance target system function below the level of injury. Also, exercise for those with SCI has potential benefits of developing muscle, bone and enhancing blood circulation.3 Exercise for SCI patients can prevent muscle atrophy and complications by increasing oxygen uptake and vital capacity, and improving muscular strength and cardiovascular function.4 Rowing has been suggested as an activity that provides multiple movements for improving muscle balance in the rotator cuff in people with SCI.5,6
Upper extremity exercise in SCI patients includes the use of an upper extremity ergometer4,7,8 and a wheelchair ergometer,9-11 whereas, lower extremity exercise includes cycles that use electrical stimulation such as functional electrical stimulation (FES). Upper and lower extremity exercises included a combination of exercises with a rowing ergometer.4,5,12
In general, rowing exercises require a strong physical condition for fast muscle contraction that can be related to the mobilization of anaerobic energy sources which is higher than other exercises.13 In a previous study,5,14 FES-assisted rowing device ROWSTIM (Therapeutic Alliances Inc., OH, USA) had been reported to be safe and effective for the improvement of cardiorespiratory fitness in SCI patients. This rowing exercise combines upper and lower extremity movement, and has special break apparatus for the FES to work on hamstring and gluteus muscles. In addition, the equipment only adjusts the FES response after a period of time SCI patients spent practicing with the FES response. It is operated by a FES button which is gripped and controlled by the patient.5 However, SCI patients who show no FES response cannot perform rowing. Furthermore, due to fast muscle fatigue from FES, SCI patients must limit the amount and duration of performing rowing exercise.15 Accordingly, we have developed a motor driven rowing device MotorROW (SeedTech, Incheon, Korea) (Fig. 1) based on the Concept2 rowing model E (Concept2 Inc., Morrisville, USA).16,17
Rowing with the MotorROW can be used by patients with muscle fatigue from FES and insufficient muscle strength. It is designed with a motor-driven seat that moves backward and forward and is adjustable according to a patient's leg length. It does not require a practice training period to respond to FES and a separate switch to control the operations of to contraction muscle. Even in SCI subjects with complete injury, MotorROW allows for the natural movement of rowing similar to healthy subjects.
We conducted this study to investigate the differences of cardiorespiratory responses such as oxygen consumption, respiratory exchange ratio, heart rate, metabolic equivalents and rate of perceived exertion on SCI paraplegic patients undergoing an exercise stress test with upper extremities rowing only, and with FES lower extremities rowing.
MATERIALS AND METHODS
Subjects
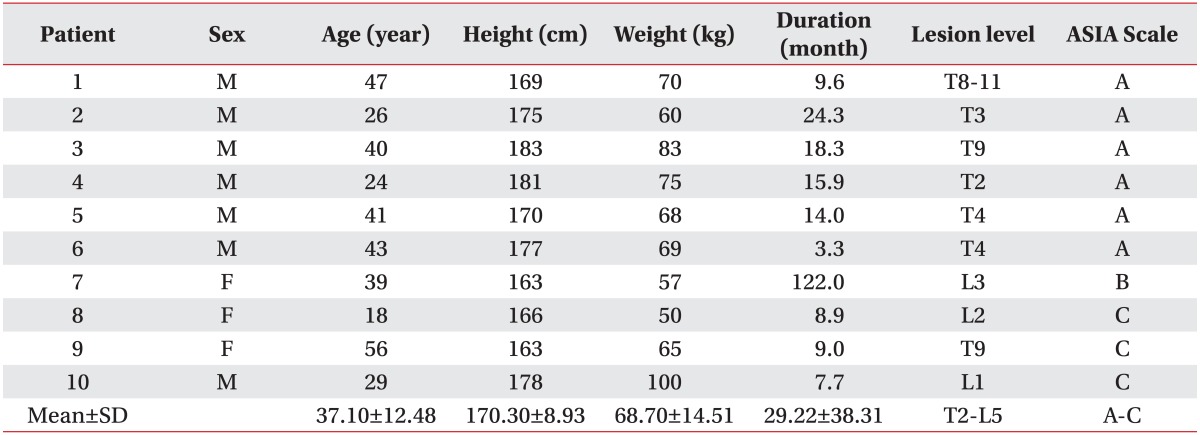
Ten paraplegic SCI patients participated in upper extremities rowing only and upper and FES lower extremities rowing. The level of injury ranged from lumbar (n=4) to thoracic (n=6). The institutional review board of National Rehabilitation Center of Korea approved the methods of this study. All subjects participated in this study after submitting an informed consent form with adequate explanation. Subject characteristics are presented in Table 1.
SCI patients whose injuries occurred at least three months prior to the start of the study were selected as subjects. Patients who had limited passive range of motion, cardiopulmonary disease, lower extremity fracture, dislocated hip, or pressure ulcers were excluded.
Measurements
A portable K4b2 gas analyzer (COSMED, Rome, Italy) was used for the analysis of respiratory gas. Heart rate (HR) was recorded using a portable heart rate monitor (Polar Beat, Port Washington, NY, USA). Analysis of respiratory gas was performed along with rowing; the experiment began when the subjects' respiratory gas data was stabilized after resting.
The work rate (WR), oxygen uptake per kilogram of bodyweight per minute (VO2
peak and VO2
mean), respiratory exchange ratio (R), HR and metabolic equivalents (METs) were measured in real time during the examination. In addition, the rate of perceived exertion (RPE) was measured immediately after examination using the Borg RPE scale.18 The possible scores for RPE ranged from 6 (no exertion) to 20 (very strong exertion).
The criteria for a patient reaching VO2
peak were as follows: VO2 plateau achieved, despite an increased exercise intensity; R>1.15; HRpeak achieved (220-age) when estimated with Karvonen's age; and detected RPE of 19-20 grade.19,20 If one or more of these parameters exceeded the criteria, it was assumed that VO2
peak had been achieved. If one of these criteria were not met, it was considered an early termination. When WR was not maintained for at least 15 seconds at the corresponding stage or if a subject wished to terminate the examination, the exercise examination was discontinued.
Data for the analysis of respiratory gas was measured in real time and was then analyzed with an interval of 30 seconds to calculate the mean and peak value of each variance.
Experimental procedure
The subjects given instructions how to use each piece of rowing equipment and were asked to spend approximately 5 minutes rowing comfortably for at least one day prior to the exam. Two different rowing tests were randomly assigned to each participant, which were performed at least one day apart. Each rowing began with 20 W, and its intensity increased each 10 W every two minutes, resulting in a graded exercise test. Subjects were encouraged to exercise as long as possible.12 The subjects with SCI rowed at a self-selected stroke rate.
Fixed rowing ergometer (fixed rowing)
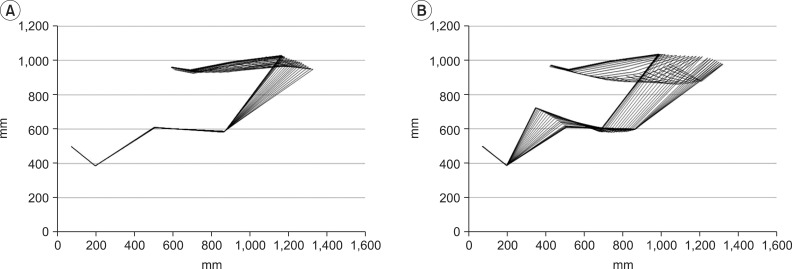
Fixed rowing involves the use of the upper extremities only on MotorROW without seat movement or FES; the lower extremities did not move (Fig. 2). The exercise stress test was conducted using the upper extremities only with a chair fixed at a position that was the most comfortable to the subject.
Motor rowing ergometer (motor rowing)
MotorROW consisted of a chair with inclination control, control system, button controller, leg supporter, safety belt, and seat. The inclination control on the chair allowed for trunk flexion and extension in accordance with the rowing motion and was designed to control the range of motion; the upper and lower extremities could move (Fig. 2). The motor control system included a control box and program, which allowed the patient to control the speed as well as the start- and end-point according to their leg length. Start and stop buttons were installed on a button controller on the handle to control movement of the seat, and a hold button was installed in the center of the grip. A seat and safety belts were developed to allow for lowered pressure on the buttocks and trunk and trunk stability for SCI. For the SCI patients who showed insufficient response to FES to near full knee extension, the exercise stress test was conducted using motor rowing alone without applying FES. The 4-channel FES stimulator (MEGA XP, Cybermedic, USA) has been mounted on the MotorROW. Electrical stimulation (monophasic rectangular phase, 30 Hz, 10 to 140 mA) was applied through a surface electrode to the hamstring and quadriceps muscles in drive and recovery phases of the rowing cycle. The synchronization of FES and the seat was automatically controlled so the position of seat on the rail with mounted optical encoders.21
Statistical analysis
SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Wilcoxon signed rank test was conducted to compare fixed rowing with motor rowing in all SCI patients. For all data, the mean and standard deviation of each factor were calculated using descriptive statistics. The statistical significance level was set as p<0.05.
RESULTS
An exercise stress test was conducted on participating SCI patients using fixed rowing and motor rowing to measure cardiopulmonary responses such as exercise time, VO2
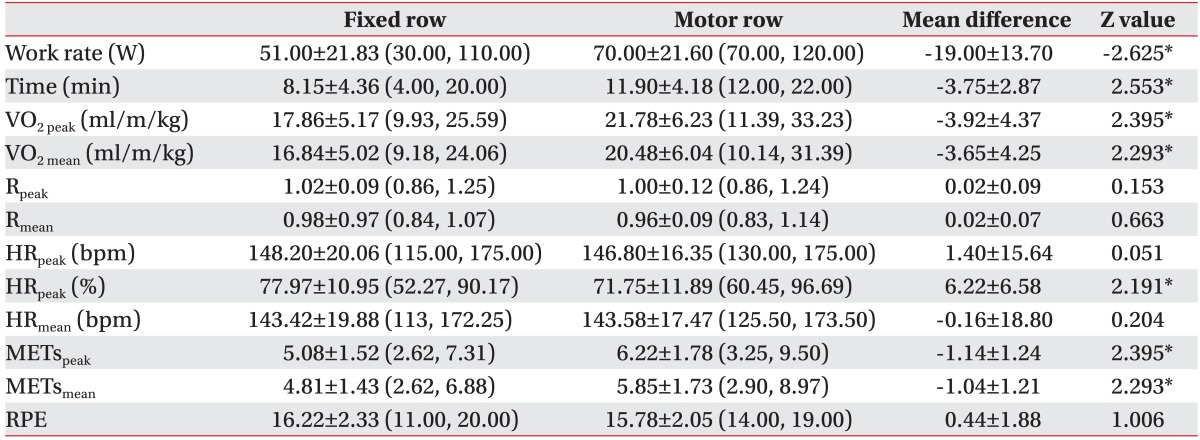
peak and HR. The results of the exercise stress test conducted on all subjects under the two different conditions are presented in Table 2. WR and exercise time were significantly higher in motor rowing than in fixed rowing. VO2
peak, VO2
mean, METspeak, and METsmean were also higher in motor rowing than in fixed rowing. R, HRpeak, HRmean and RPE were not significantly different in patients after either rowing test. However, the percentage value after dividing the HRpeak (%) measured by Karvonen's estimated HRpeak (220-age) was significantly lower in motor rowing than in fixed rowing, and was greater than 70%.
DISCUSSION
In healthy adults, rowing is an effective exercise method as compared to other combined exercises such as FES cycle with arm crank exercise (ACE). In SCI paraplegic patients, rowing has been recommended to reduce patient risk factors for coronary artery disease, increase leg extension power,16 and significantly increase VO2
peak and HRpeak.8
In this study, exercise with the MotorROW is presented as a method to prevent complications that occur due to the lack of exercise in patients with SCI. Also, the effects of exercise using fixed rowing and motor rowing were compared. Muscle contraction of lower extremities in rowing exercise allows for the movement of the seat. Generally, the fixed rowing method is an indoor form of exercise for the disabled that uses the muscular strength of the upper extremities alone with the seat in a fixed position. This study validated MotorROW as an exercise apparatus in patients with paraplegic SCI by comparing the effects of cardiopulmonary responses such as VO2, HR and METs between the currently used fixed rowing in SCI and the recently developed motor rowing for patients with SCI.
One of the most significant advantages of the MotorROW allows for a natural repetitive rowing motion like a healthy person and continuous passive movement in the lower extremity, even in patients who do not show sufficient responses to FES. In our study, the quadriceps muscle of six patients with complete SCI did not show response to FES. These subjects needed an assistive device to make a movement like an electric motor that can assist FES or replace FES. In this study, all subjects have experienced upper and lower extremity exercises in the first session by the MotorROW.
Presently, WR, time and cardiorespiratory response factors such as VO2
peak, VO2
mean, METspeak, METsmean were significantly higher in motor rowing than in fixed rowing in our study. In a prior study that assessed upper extremity exercise stress tests in patients with SCI, WR was reported to be 57±5 W.22 WR in the present study showed significantly higher (70±21 W) in motor rowing than in fixed rowing (51±21 W). WR and time during the motor rowing exercise test was 37.3%, which was 46.0% higher than that during fixed rowing.
The reported range for VO2
peak values after an upper extremity exercise stress test and fixed rowing in patients with SCI is 11.20±5.1 ml/m/kg23 to 24.12±2.60 ml/m/kg.24 In our study, VO2
peak during motor rowing was 21.78±6.23 ml/m/kg. VO2
peak values in the motor rowing exercise test increased about 21.9% more than fixed rowing. In a previous study,4 using upper and lower extremity exercise equipment, VO2
peak in five patients (lesion level C7-T5) after FES cycle with ACE was 25.38±6.03 ml/m/kg and VO2
peak after FES-assisted rowing was 25.62±2.98 ml/m/kg. In the study, compared rowing ergometer and treadmill running, the increased VO2
peak and the attenuated HR during rowing indicated the involvement of more muscle, facilitates the venous return and elevates the central blood volume.20
HRpeak (%) for motor rowing was significantly lower than that in fixed rowing, while WR, exercise time, VO2, and METs were significantly higher in motor rowing than in fixed rowing. These results indicate that the increased exercise time for patients performing motor rowing was associated with a decreased burden on the heart and body compared to that of fixed rowing.
The main characteristic of recent recommendations on physical activity based on METs is that health benefits can be achieved by moderate intensity. Absolute intensity of METs was defined as a moderate exercise of Center for Disease Control (CDC) and The American College of Sports Medicine (ACSM) corresponding to 3-6 METs.25 Therefore, although relative METs among patients can be compared only broadly, METs peak were 5.08±1.52 in fixed rowing and 6.22±1.78 in motor rowing (22.4% increase) based on absolute intensity. While the difference between the rowing tests was statistically significant, the data indicates that motor rowing is suitable for moderate intensity or higher maximal exercise.
RPE, defined by Borg,18 is used to document a patient's exertion during a test. As RPE is correlated with HR and oxygen uptake, it is used as a predictor of exercise intensity. ACSM recommends that RPE should be widely used as an index to monitor exercise intensity. The target RPE for aerobic exercise is recommended as 16-18.26,27 In our study, RPE was 16.22±2.33 in fixed rowing and 15.78±2.05 in motor rowing, very similar to the published values (17.3±3.01) for patients with T1-T2 paraplegia using upper extremity exercise equipment.23 Despite similar RPE scores between the two tests in our study, the variables (WR, time) in the motor rowing exercise test represent a significantly higher-degree compared to the fixed rowing test.
Safety was of the important concern in these studies, which included the electrical system, lower-extremity injury within the knee and ankle, and the risk for ulcer development.5 During the tests, no advert events occurred with this device and were no instances of electrical-related issues, lower extremity at knee and ankle joint, and no ulcer development.
Taken together, the results of our study indicate that motor rowing is the more appropriate exercise than fixed rowing. If the MotorROW is actively used as equipment for training or exercise equipment in the future, it could be used as an appropriate apparatus for eliciting the cardiorespiratory responses in patients with SCI.
A limitation of this study was the small number of subjects. The results of this study were confused by the effects of FES leg movement with passive leg movement by motor, because the subjects who have voluntary leg muscle contraction in neurologically incomplete SCI also participated. Further study will be required to observe improvements of functional outcomes such as oxygen uptake and heart rate after MotorROW training in patients with SCI.
The results of our study indicate that the exercise method using MotorROW for paraplegia SCI may be more efficient for positive change in the VOpeak, HR and METs than fixed rowing.
CONCLUSION
Exercise effects were compared between fixed rowing and motor rowing to optimize the apparatus for VO2, R, HR, METs and RPE responses for SCI patients. Exercise stress tests were conducted for 10 SCI (ASIA A-C) patients using two rowing methods. WR, exercise time, VO2, and METs were higher, and HR was lower in patients with SCI after motor rowing than after fixed rowing.
MotorROW has an advantage of allowing natural rowing motion and passive leg movement as well as providing the significant change of cardiorespiratory exercise variables even for paraplegic SCI without lower extremity motor function. It is an acceptable and safe exercise device to promote motivation in cardiovascular fitness for SCI patients.

 XML Download
XML Download