

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Appreciating that the elderly have their own personal desires and deserve to be treated respectfully, we cannot improve the quality of life of the elderly without considering sex, which is one of the basic instincts of human beings. Traditionally in Korean society, it has been considered shameful to discuss the sexual life of older people. However, the introduction of Western cultures and liberalization has made the old younger, not only physically but also mentally, and this causes another kind of social problem related to the breaking down of social conventions about expressing sexual desire.1-3
According to the results of the Global Study of Sexual Attitudes and Behavior conducted between 2001 and 2002 for 27,500 men and women in their 40s to 80s, in Korea, 98% of men and 89% of women in their 50s, 95% of men and 68% of women in their 60s and 89% of men and 50% of women in their 70s replied that sexual intercourse is still important in their lives, and they answered that the biggest benefit of sex is that it helps them feel a sense of closeness with their own partners mentally and physically and maintain their relationship.4,5 Recently, on the men's side, remarkable research has been performed and treatments have been developed, and they have contributed to improving the quality of men's lives. However, although a high prevalence rate of female sexual dysfunction has been reported, not enough research on this matter has yet been performed.6-8
In Korea, it is not easy to investigate the actual conditions of older people's sexual life due to the influence of their traditional culture, and therefore, studies on this matter have been relatively insufficient. This study is a basic survey of the sexual life of the elderly of Korea, a country that has become an aging society. In this study, we investigated the patterns of the sexual life of the old who visited senior welfare centers of district offices of Seoul.
MATERIALS AND METHODS
This study was conducted between May, 2009 and October, 2009 for 154 men and 299 women over 60 years old who visited the senior welfare centers of 7 district offices of Seoul and participated voluntarily in the survey. All the visitors submitted the consent form.
For males, we did a survey of the frequency of sexual intercourse, sexual desire, reasons for not having sex, the treatment of impotence, and the history of venereal diseases and International Index of Erectile Dysfunction-5 (IIEF-5).9-11 For females, we also did a survey of the frequency of sexual intercourse, sexual desire, reasons for not having sex, difficulty of sexual intercourse, and the history of venereal diseases.
In addition, to investigate Lower Urinary Tract Symptoms (LUTS), which is one of the most common diseases of the elderly, we administered the International Prostate Symptom Score (IPSS)12 for the males and Overactive Bladder Symptom Score (OAB-SS) and International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF)13-15 for the females.
We used Student's t-tests or Mann-Whitney tests for continuous variables and chi-squared tests for non-continuous variables. For the correlation with LUTS, we used correlation analysis. To analyze all of the statistical data, we used SPSS 19.0 (SPSS Inc., Chicago, IL, USA) and regarded p<0.05 to be statistically meaningful for this study.
RESULTS
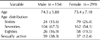
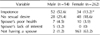
Among the 154 males, 24 (15.6%) were in their 60s, 104 (67.5%) in their 70s, and the other 26 (16.9%) in their 80s, and their average age was 74.5. 62.5% of them in their 60s, 38.4% in their 70s, and 15.3% in their 80s were sexually active. Among all of them, 59 (38.3%) were having sexual intercourse on an average of 2.03 times a month (Table 1, Fig. 1). The other 95 (61.7%) males were not having sexual intercourse because of impotence for 52 (52.6%), no sexual desire for 28 (29.4%), and the sexual partner's problems for the other 15 (15.7%) (Table 2). 6 (6.3%) had 2 factors at once, and 1 (1%) had 3 factors at the same time. Among all the males who had sexual intercourse, 2 (3.4%) did not have spouse, and among who did not have sexual intercourse, 11 (11.6%) did not have a spouse. Among 34 of them who were under treatment for impotence, 28 (82.4%) were taking impotence drugs, 2 (5.9%) were having injections, 1 (2.9%) had surgery for impotence, and the other 3 (8.8%) received other treatments. 15 (53.6%) bought oral impotence drugs in drugstores after a doctor's prescription, while the other 13 (46.4%) bought them without a prescription. Among the males who bought the drugs without a prescription, 5 (34.7%) bought them in drugstores, while the other 8 (65.3%) bought them through unofficial channels. The reasons why they did not treat their impotence were no sexual desire for 17 (53.1%), financial hardship for 7 (21.9%), poor health for 3 (9.3%), and other reasons for the other 5 (15.7%). The sexual partner's problems consisted of spouse's poor health for 7 (46.7%), spouse's lack of interest in sexual intercourse for 5 (33.3%), not having a spouse for 2 (13.3%), and other problems for 1 (6.6%).
64 (41.6%) of them had experienced sexual intercourse with other partners than their own spouses. Among the 46 (29.9%) males who had experienced venereal diseases, 35 (76.1%) had experienced (gonococcal or non-gonococcal) urethritis, 6 (13.1%) experienced skin diseases such as pubic lice, and 5 (10.8%) had experienced syphilis.
The IPSS score was an average of 10.48, and the higher IPSS was, the lower IIEF-5 was. (The correlation coefficient was -0.183 p=0.035) (Fig. 2).
Among the 299 females, 79 (26.4%) were in their 60s, 162 (54.1%) in their 70s, and the other 58 (19.5%) were in their 80s, and their average age was 73.4 (Table 1). Among 41 (13.7%) of them who had sexual desire, 37 (12.4%) were actually sexually active, and 30 (81%) of them had sexual intercourse once a month on average. The average age of the females who were sexually active was 69.5, while that of the others who did not was 73.9, which shows that age influences sex life (p<0.001). Among the 37 females who had sexual intercourse, 35 were under 75 years old (94.6%) (Fig. 1). 12 (32.4%) reported difficulty having sex because of a lack of sexual desire, 11 (29.7%) because of not taking pleasure in having sex, and 9 (24.3%) because of no sexual arousal, which shows that most of the females had sexual arousal disorders. 4 (10.8%) of them had dyspareunia, and 1 (2.7%) had another disorder (Fig. 3). 163 (63.2%) answered that they did not have sexual intercourse because of a lack of a sex partner, 48 (18.6%) because of no sexual desire, 34 (13.2%) because of the sex partner's impotence, 10 (3.9%) because of the sex partner's poor health, 3 (1.1%) because they thought it would be harmful for their health, and the other 4 (1.5%) for other reasons (Table 2). 13 (5%) had 2 factors at once, and 1 (0.4%) had 3 factors. Among all of the females who were sexually active, 17 (45.9%) did not have a spouse, and among who did not have sexual intercourse, 163 (63.2%) did not have spouse.
Among 23 of them who had experienced venereal diseases, 13 (56.5%) had experienced urethritis, 5 (21.7%) had experienced skin diseases such as pubic lice, 3 (13.1%) had experienced syphilis, and 2 (8.7%) had experienced other diseases.
The ICIQ-SF was on average 2.39. 135 (45.2%) reported that they did not have incontinence, while 66 (22.1%) answered that they had experienced incontinence before arriving at the toilet, 46 (15.4%) when putting on clothes after having a leak, 18 (6%) in their sleep, 14 (4.7%) all the time, 8 (2.7%) when coughing, and the other 2 (0.7%) without any particular reason.
According to the OAB-SS, 71 (23.7%) had no subjective symptoms, while the other 228 (76.3%) had at least one subjective symptom. An average of 1.05 items of the overactive bladder self-diagnosis questionnaire applied to the females who were having sexual intercourse, while 2.43 items applied to those who were not, which shows that overactive bladder was related to their sex life (p<0.001).
DISCUSSION
Since Kinsey's research on sex conducted in 1953, various studies on sex have been made from the perspective of sociology and psychology. In the clinical fields, psychiatrists and clinical psychologists have also developed sexual medicine.16 It is known that the sexual development of human beings continues throughout their lives and that this is significantly associated with changes in biological, psychological, and social factors.
The result of this study shows that 38.3% of elderly men have sexual intercourse, while only 12.4% of elderly women do, which is a much lower percentage compared to men. This may be because men have had more sexual intercourse with other sex partners besides their own spouses. In addition, the percentage of older men that have their own spouses still alive is higher than that of older women. However, a number of them reported not having sexual intercourse with their own spouses but with other women, and this suggests that we need to show greater concern for sexually transmitted diseases in the elderly.
For older men, the most basic reasons for not having sex were related to their own sexual problems such as impotence and sexual desire, while for older women, the reasons were related to their partner's problems such as no spouse and spouse's impotence. A majority of the men with impotence bought oral impotence drugs without a doctor's prescription, which shows that the purchase of medicine through illegal channels has reached a very serious level.
According to the results of a recent survey of the actual conditions of sex life conducted in Jeju Island, Korea with about 350 elderly men and women, 63.8% of men and 27.6% of women reported that their sex life was important to them, and 8.1% of men and 1.6% of women had used prostitution to satisfy their sexual desire.17 However, in Korea, elderly men's prostitution has been reported on by the media, and this has had a negative influence on their social and psychological position, weakening Koreans' traditional respect for the elderly as well as causing medical problems for them. Korean society has a particularly conservative view on old people's sexual behavior, and there is a great difference between the ideal and the reality of their sex life. This makes it very difficult to understand sexual problems in the elderly.
In the case of voiding symptoms, the higher the men's IPSS was, the lower their IIEF-5 was, and only a few items of the OAB-SS applied to older women who were having sexual intercourse, which shows that, for both men and women, voiding symptoms have an inverse correlation with sexual activity. The lack of confidence in their bodies could be a cause for the lack of the interest in sex and the evasion of sexual intercourse.
In spite of the high prevalence rate of LUTS and sexual dysfunction in older people, the correlation between the two has been controversial. The Massachusetts Male Aging Study, which was a large-scale study, reported that 34.8% of erectile dysfunction occurred in patients in their 40s to 70s, but no potential correlation with LUTS was considered.18 However, a number of recent studies have suggested that there is an important correlation between LUTS and men's sexual dysfunction. In thei research of Frankel et al on 423 British men over 40 years old, men who suffered from LUTS had negative trends in sexual functioning, and higher odds ratios of sexual dysfunction were found in those with LUTS, especially storage symptoms associated with incontinence. The result of another study on 2011 Frenchmen in their 50s to 80s conducted by Macfarlane et al also suggested that voiding symptoms have an inverse relation with satisfaction with one's sex life and frequency of sexual intercourse.18-22
64 (41.6%) of the males in our study had experienced sexual intercourse with other partners besides their own spouses, and 46 (29.9%) had experienced venereal diseases, while 23 (7.7%) females had experienced venereal diseases. There is a significant gap between men's and women's venereal disease morbidity rate, and it is thought that this may be associated with the frequency of older men's sexual intercourse with other women besides their own spouses. According to the National Health Insurance Corporation's analysis on health insurance payments between 2006 and 2010, patients who received treatments for venereal diseases had increased by 1.4% a year on average from 333,000 patients in 2006 to 352,000 patients in 2010. The result of age-specific analysis shows that the rate of the average annual increase has dropped for patients in their 30s and 40s, while the rate has been increasing for patients in their teens, 20s, and 50s, with a greater than 6% increase for patients over 60 years old. This is because the aging population is increasing, and widespread availability of impotence drugs has resulted in the increase in sexual activity. Furthermore, venereal disease education for old men and women has been insufficient. Therefore, we need to provide more education and care targeted at their age group.
CONCLUSIONS
According to the results of this study, 38.3% men and women over 60 years old are sexually active, and voiding symptoms are associated with impotence.
In the case of the older women, 12.4% of them have sexual intercourse, and overactive bladder has a strong influence on their sex life. Considering that sexual arousal disease is a significant cause of having difficulty enjoying sex life and that for many older women, the most basic reason they do not have sexual intercourse is because they have no sex partner, they deserve more attention and support from society.



 XML Download
XML Download