

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Particulate bone material with varying particle sizes has been used extensively in the dental field for restoring alveolar bone deficiencies [1]. Particulate bone material tends to be used especially frequently in guided bone regeneration [2]. The method used to apply bone particles to the recipient site appears to be quite simple: the material is placed onto the recipient bed and then packed and protected with the aid of a membrane. However, this seemingly simple procedure frequently becomes complicated due to the specific morphology of a bone defect, which can vary widely [3,4]. In particular, uncontained types of defects (i.e., those lacking a surrounding bone wall to stabilize the graft) may render bone particles unstable, thereby increasing the technical difficulty, surgical time, and potential for surgical error. The worst-case scenario with respect to error is displacement of the bone particles, which can lead the regenerated bone to take on an undesired shape or cause the loss of a large proportion of the grafted bone particles.
Three-dimensional bone blocks were developed in order to address these drawbacks. Bone graft material from an autogenous source is regarded as the gold standard, but autogenous bone blocks have a high resorption rate, are associated with donor-site morbidity, and are usually only available in quantities that are insufficient for treating large defects [5]. Alternatives include allogenic, xenogenic, and synthetic bone blocks [6,7,8,9], but the evidence regarding the clinical efficacy of these alternatives remains limited.
Synthetic bone blocks made of calcium phosphates (CPs) have been investigated in a few studies, and promising results have been demonstrated in vertical augmentation and circular defect models of rabbit calvaria [6,8,10]. In terms of new bone formation, blocks made of monophasic CPs (i.e., hydroxyapatite [HA] and tricalcium phosphate [TCP]) have been reported to be inferior to those made of biphasic CP (BCP; i.e., combinations of HA and TCP) [6]. While the use of HA or TCP alone is associated with problems such as an imbalance between new bone formation and space maintenance, due to the resorption characteristics of each material [6], BCP is known to be able to promote both simultaneously. Moreover, the reactivity of BCP can be modified by changing the HA:TCP ratio [11].
Ideally, synthetic blocks grafted into defects should ultimately be replaced by newly formed vital bone. From a practical viewpoint, the synthetic grafted block must be infiltrated by newly formed bone, whereby a solid bridge of living bone tissue forms in the residual graft, ensuring long-term stability and function. Bone infiltration is known to depend largely upon the pore structure of the block [12]. In particular, the three-dimensional interconnectivity and porosity are known to be significantly affected by the processing method used in the production of the material [12,13]. Therefore, one of main themes in the development of synthetic bone substitutes has been the optimization of the physical pore structure [13].
Several processing methods, such as the sol-gel, foaming, and replica methods, have been introduced for producing BCP [12]. However, synthetic bone blocks are more difficult to process in a way that ensures proper functionality than is particulate synthetic bone. BCP blocks processed by different methods have been shown to behave differently in vivo. Kim et al. [14] implanted BCP blocks and particulate BCP into rabbit calvarial defects and found a limited amount of newly formed bone inside the BCP blocks, whereas interconnecting bone had formed in the particulate BCP. Moreover, the addition of bone morphogenetic protein 2 did not enhance the growth of new bone into the BCP blocks. However, Hwang et al. [6] observed remarkable bone ingrowth into BCP blocks.
Extrusion with polymethylmethacrylate beads as a pore former is known to be more convenient than other processing methods and also allows the production of larger pieces of porous synthetic bone []. In addition, this method not only produces a homogeneous pore distribution, but also allows the pore size to be controlled. However, it has been pointed out that the conventional extrusion method is not appropriate for the production of blocks with interconnected pores, and a modified extrusion method was therefore proposed [15]. This modified method involves reacting dicalcium phosphate dehydrate (DCPD) with calcium nitrate tetrahydrate (CN) in combination with a piston-and-screw-type extrusion system. This technique has been shown to result in increased pore interconnectivity, and the resulting BCPs were found to vary in both porosity (56%-88%) and compressive strength (0.5-10.5 MPa) depending upon the extrusion type and the HA:TCP ratio.
The aim of this study was to characterize the properties of BCP blocks processed using the modified extrusion method and to determine the osteoconductive potency of the blocks in a standardized rabbit calvarial defect model.
MATERIALS AND METHODS
Preparation of the BCP blocks
The details of the processing method are available elsewhere [15]. In brief, HA [Ca10(PO4)6(OH)2, Junsei, Tokyo, Japan], DCPD [CaHPO4·2H2O, Junsei, Tokyo, Japan], CN [Ca(NO3)2·4H2O, Duksan Pure Chemicals, Ansan, Korea], and polymethylmethacrylate beads [(C5O2H8)n, Junsei, Tokyo, Japan] were used to fabricate porous BCP blocks with different HA:TCP ratios. HA and DCPD were first mixed in different ratios, and then the CN solution and binder were added to the powder mixture. The mixtures were kneaded to make a dough-like slurry, which was vacuum-packed and stored for one day to allow homogeneous distribution of the moisture and binder. The slurry was extruded into cylindrical rod samples using a screw-type extruder. Cracking of the extruded rod-type samples was avoided by drying them in a humidity chamber at 90℃ and 70% relative humidity for one day, and then in a drying oven at 100℃ for one day to remove the remaining moisture. The dried samples were sintered at 1,250℃ for five hours and then cooled in the same furnace. The sintered rod samples were cut into disk-shaped samples with a diameter of 8 mm and a height of 3 mm. BCP blocks with three HA:TCP ratios were made:HA8 (8:92), HA48 (48:52), and HA80 (80:20).
Characterization of the BCP blocks and phase analysis
The apparent density of the sintered BCP disk samples was measured, from which the porosity was calculated. The microstructure of the disk samples was observed using scanning electron microscopy (S-4200, Hitachi, Tokyo, Japan). The HA:TCP ratio in the BCP samples was analyzed using X-ray diffractometry (X'pert MPD-PRO, Panalytical, Almelo, The Netherlands), which was carried out at 40 kV and 30 mA with a copper target. The compressive strength of the BCP disks was evaluated using a universal test machine (Testometric M350-10CT, Lancashire, England (500 kgf load cell, 0.5 mm/min crosshead speed).
Animal experiments
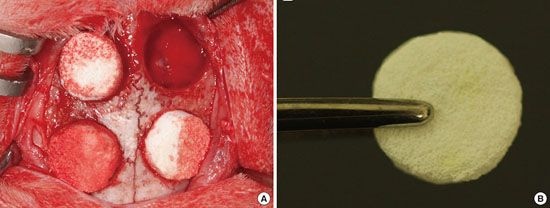
Twelve adult New Zealand white rabbits (2.5-3.5 kg) were used in this study. This animal research followed protocols approved by the Institutional Animal Care and Use Committee, Yonsei Medical Center (approval no. 2012-0093-3). General anesthesia was induced by the intramuscular injection of a mixture of ketamine hydrochloride (Ketalar, Yuhan, Seoul, Korea) and xylazine (Rompun, Bayer Korea, Seoul, Korea). The operative site was shaved and rinsed with povidone-iodine. Local anesthesia was administered by injecting 2% lidocaine HCl (Huons, Seoul, Korea) via a dental syringe. A sagittal incision was made along the midline of the calvarium, followed by elevation of a full-thickness flap. Four circular osteotomies with a diameter of 8 mm were performed using a trephine bur under saline irrigation. One defect in each animal served as a control and was filled with blood coagulum. The three remaining defects received one of the three types of BCP block (i.e., HA8, HA48, and HA80). The blocks were fitted into the osteotomy such that no spinning movement was observed. The flaps were then repositioned without tension and sutured with 4-0 Monosyn (B-Braun, Aesculap, Center Valley, PA, USA; Fig. 1). The animals were sacrificed at either two weeks (n=6) or eight weeks (n=6) postoperatively.
Histologic processing
Block sections of the surgical sites, including the adjacent tissue, were removed and immersed in 10% formalin for 10 days. They were then rinsed in sterile water and immersed in 5% formic acid for 14 days, then trimmed, dehydrated, and embedded in paraffin. Serial 5-µm-thick sections were cut through the center of the circular calvarial defects. Sections from each block were stained with hematoxylin-eosin and Masson's trichrome stains, and the two central most sections were subjected to histologic and histomorphometric analysis.
Histologic and histomorphometric analyses
The histologic slides were examined using a binocular microscope (Leica DM LB, Leica Microsystems, Wetzlar, Germany) equipped with a camera (Leica DC300F, Leica Microsystems, Wetzlar, Germany), and images of the slides were captured using a slide viewer program (BX50, Olympus, Tokyo, Japan) on a computer connected to the microscope, and saved as TIFF files. Histometric measurements were made using an automated image-analysis system (Image-Pro Plus, Media Cybernetics, Silver Spring, MD, USA) by a single examiner who was blinded to the treatment (i.e., control, HA8, HA48, or HA80). Two parameters were measured: the percentage of newly formed bone (%NB) and the percentage of residual BCP material (%RM).
Statistical analysis
Statistical analysis was conducted using commercially available statistical software (SPSS version 20.0, IBM Corp., Armonk, NY, USA). The descriptive data are presented as mean±standard deviation values. The Shapiro-Wilk test was performed to check for conformity with a normal distribution, the Friedman test was applied to test for statistical significance in changes between healing periods, and the post-hoc Dunn-Bonferroni method was used to test for statistically significant differences among the groups. The Wilcoxon rank-sum test was used to compare the histometric values at two and eight weeks. The threshold for statistical significance was set at P<0.05.
RESULTS
Characterization of the BCP blocks
The X-ray diffractometry patterns of the HA8, HA48, and HA80 samples are shown in Fig. 2. Both HA and β-TCP peaks were observed in all three samples; however, weak α-TCP peaks were also observed in the HA8 and HA48 samples. The contents of the crystalline phases of the samples are shown in Fig. 3.
Scanning electron microscopy revealed the presence of a three-dimensional, uniformly distributed, partially interconnected porous microstructure in the sintered BCP samples (Fig. 4). The pore size of the three samples varied according to the HA:TCP ratio, which was in turn related to the HA and DCPD mixing ratio. The pores were larger in the HA8 sample than in the HA48 and HA80 samples. The average pore size of the three types of BCP samples was 140-170 µm.
The compressive strength and porosity of the BCP blocks are presented in Fig. 5. Compressive strength increased and porosity decreased as the percentage of HA in the BCP increased. Hence, an inverse relationship between compressive strength and porosity was found. The porosities of HA8, HA48, and HA80 were >80%, ~80%, and >70%, respectively. The compressive strength of the blocks was 4-9 MPa.
Clinical findings
No adverse signs or complications were observed throughout the entire healing period. Visual inspection was performed while harvesting the tissue sections from the surgical sites. The implanted blocks were found to be in place, with no displacement evident at any of the sites, and no visual signs of infection or inflammation were observed.
Histologic findings
At two weeks
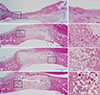
Unlike the experimental groups, structural continuity was not maintained in the control group. The defect in the control group was depressed as a result of soft tissue collapse, and new bone was mostly found at the periphery. In the experimental groups, the block bone grafts were tightly incorporated within the defects and were surrounded by soft tissue and dura mater. The blocks appeared to have mostly maintained their original shape and size. Although the border of the blocks became irregular during the healing period, they were clearly distinguishable from the native bone. New bone was observed on the blocks, adjacent to the defect margin. The degree of infiltration of new bone tissue into the block varied, but new bone tissue was generally confined to the border of the block and was more prevalent in the lower part of the block than in the upper part. The degree of infiltration was similar among the HA8, HA48, and HA80 groups (Fig. 6).
At eight weeks
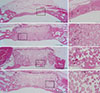
Structural depression was still observed in the control group after eight weeks of healing. Thin new bone extended from the defect margin, and bone islands were found between the margins in some specimens. In the experimental groups, bone infiltration had progressed horizontally to the center of the block. The bone formation in the vertical direction was markedly different from that found in the horizontal direction; minimal bone formation was noted adjacent to the periosteum, and a thin lining of bone could be observed along the dura mater. Resorption of the block progressed at the border between the block and the native bone, such that the native bone was well incorporated into the edge of the block. The amount of resorption appeared to be greater and the edge of the block seemed more intermingled with native bone in the HA8 group than in the HA48 and HA80 groups. The lacunae of the new bone contained osteocytes, and osteoblasts were observed lining the pores; however, very few reversal lines were seen. The infiltration of inflammatory cells was observed in the fibrous tissue lying over the block (Fig. 7).
Histomorphometric findings
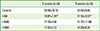
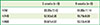
The histometric findings are presented in Tables 1 and 2. At both healing points, %NB was greater in the control group than in any of the experimental groups. The %NB in the control group was significantly different from the %NB observed in the HA8 group at both healing points, but was not significantly different from the %NB values in the HA48 and HA80 groups. There was no significant difference in %NB among the HA8, HA48, and HA80 groups, or between two and eight weeks of healing within a given group.
%RM was slightly greater in the HA48 and HA80 groups than in the HA8 group at both healing time points, but the difference did not reach statistical significance. No significant differences were found regarding this parameter between two and eight weeks in any of the experimental groups.
DISCUSSION
The block-type bone substitute is advantageous over the particulate type with respect to manageability, the ability to maintain the shape of the space, and the restoration of uncontained and large defects. In order to ensure correct function and a favorable long-term prognosis, the block-type bone substitute must ultimately be replaced by newly formed vital bone, or the new bone tissue must be closely interconnected within the block. The microstructural and macrostructural properties of the bone substitute should therefore be optimal for the ingrowth of new bone tissue, and these properties are determined by the processing method used in fabricating the material [12]. In the present study, block bone substitutes were produced using a modified extrusion method. While block bone with homogeneously distributed pores of a controlled size can be fabricated using the original extrusion method, this method is not appropriate for making block bone with suitably interconnected pores. However, improved pore interconnectivity was rendered possible by modifying the original method to include a reaction between DCPD and CN [15].
Examination of the mechanical and structural properties of the three types of block bone tested in this study revealed that the pore size and porosity decreased with increasing relative HA content. Pore size and porosity play an important role in bone ingrowth, because pores allow the migration and proliferation of osteogenic cells [16]. Small pores cannot contribute to bone formation, because they are infiltrated with avascular tissue instead [17]; pores with a minimum diameter of 50 µm are required for bone ingrowth [18]. Other studies have shown better bone formation when the pore size was >300 mm [19,20]. Larger pores are favorable for vascularization, high oxygenation, and subsequent bone formation, whereas smaller pores may favor osteochondral ossification. However, it has also been demonstrated that pore interconnection size is more important than pore size for bone formation [21,22]. The threshold of porosity is known to be approximately 60% [22,23], and bone substitutes with a porosity of <60% tend to have small pores and few pore interconnections [24]. In the present study, the pore size of the three block types ranged from 140 to 170 µm, and all had a porosity >70%.
The mechanical properties of BCP are known to be highly dependent upon the porosity [23,25]. Mechanical strength tends to decrease with increasing porosity, thus determining the indications for the different block bone substitutes. Bone substitutes should meet certain mechanical standards for specific recipient sites. For example, an excessive number of pore interconnections may render the block unsuitable for load-bearing areas [25]. The three blocks in the present study had a compressive strength of 4-9 MPa, which is comparable to that of cancellous bone (5.5 MPa). Considering that bone substitutes in the dental field do not require a great load-bearing capacity, the compressive strength of the three blocks was adequate for clinical usage.
Rabbit calvarial defects have been widely used for screening and evaluating biomaterials [6,10,14,26,27,28]. An ideally sized defect should exclude the possibility of spontaneous healing [26]. It has been reported that large defects, up to 17 mm×17 mm, can be created in the rabbit calvarium [29]. However, large defects prevent the creation of multiple defects in a single calvarium, making it difficult to compare various biomaterials within an individual animal and thereby making it necessary to use a greater quantity of experimental animals. Therefore, multiple smaller-sized defects are favored [6,10,14,27,28]. Sohn et al. [26] compared the healing potency of variously sized defects (6, 8, 11, and 15 mm in diameter), and concluded four 8-mm defects can be used in a single calvarium to compare the early healing process among several materials. Moreover, eight weeks of healing was found to be a suitable period for assessing the late mechanics of bone healing, such as bone maturation and graft resorption. In the present study, early and late healing periods of two and eight weeks, respectively, were selected to evaluate the osteoconductivity of three block-type BCPs of different compositions.
In all block-grafted groups, native bone was incorporated into the blocks and the initial morphology of the block was sustained, which demonstrated the space-maintaining capacity of the blocks and their resistance to tissue pressure. In contrast, the control group exhibited a depressed morphology in the defect region compared to the height of the native bone. Other block-type bones fabricated from BCP using different processing methods have been evaluated. Hwang et al. [6] and Kim et al. [14] implanted BCP blocks into calvarial defects in rabbits and found no significant changes in the augmented area between either four and eight weeks or two and eight weeks.
Space for new bone must be secured in order to ensure predictable bone regeneration, and therefore the bone morphology adjacent to the recipient bed is of the utmost importance. If bone augmentation is performed in a locally depressed area, the clinician can expect a favorable regenerative outcome. However, augmentation on a flat surface is technically difficult, and the grafted bone must withstand pressure from the overlying soft tissue. Such circumstances require space creation by affixing a tenting screw or nonresorbable membrane, especially if a particulate bone substitute is used. In the present study, the grafted block maintained its original shape throughout the two healing periods, although a portion of it was located outside of the original bony outline, indicating that modification of the block design can result in variously shaped augmentation patterns. BCP blocks also have been found to exhibit resistance against tissue pressure in a rabbit onlay graft model [10].
The theory underlying the use of BCP as a bone substitute is that new bone formation and resorption can be regulated according to the HA:TCP ratio [11]. Although the optimal ratio has not yet been determined, BCP with a high TCP content is thought to lead to greater graft resorption and concomitantly, more new bone formation. However, this concept may be challenged by the heterogeneous results of previous studies [27,28,30,31]. Some studies have found similar amounts of newly formed bone in experimental groups with different HA:TCP ratios [27,28], which is in accordance with the present study. This study evaluated the bone-forming potential of BCP with different HA:TCP ratios by producing three BCP blocks with different ratios (high, middle, and low ratios of HA to TCP), but no statistically significant differences in new bone formation were observed among the HA8, HA48, and HA80 groups.
New bone formation achieved with BCP as a block-type bone substitute is strongly influenced by pore interconnectivity [13]. If the pores are not connected with one another, fluid circulation and cell migration are interrupted, and bone tissue cannot grow into the block properly [25]. Instead, if the pores are not interconnected, bone infiltration depends on the dissolution of the block [32]. In the histologic sections examined in the present study, it was found that bone formation occurred mostly in the lower half of the blocks in all groups, with no significant difference in %NB between two and eight weeks. Kim et al. [14] reported similar histologic observations; newly formed bone was found in contact with native bone on the inferior side of the grafted block, and new bone formation in the pores increased with time. However, other studies have found significant bone formation in the center of CP blocks [6,33]. It has been clearly demonstrated that bone substitutes with small, well-interconnected pores lead to more favorable bone ingrowth than those with large and less-interconnected pores, although the two types may ultimately have a similar porosity [34]. The processing method used in this study should be further refined in order to improve new bone formation with BCP block bone substitutes.
In the present study, the grafted block was not covered by a barrier membrane. Despite the space-maintaining properties of the block, bone infiltration to the upper portion of the block was minimal and bone lining over the block was not observed. Some researchers have argued that the periosteum produces an osteoinductive signal [35], but it has been shown that the amount of bone regeneration decreases when a barrier membrane is not used [36,37]. The use of a covering membrane over the block may prevent the infiltration of soft tissue and improve bone formation in the upper portion of the graft.
In conclusion, block bone substitutes with three compositions (i.e., three HA: TCP ratios) processed by a modified extrusion method exhibited limited osteoconductive potency, but excellent space-maintaining capability. Further research is necessary to improve the processing method.





 XML Download
XML Download