

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiovascular disease is the leading cause of death in both women and men. Although the number of cardiovascular deaths has declined in men, it has actually increased in women over the past decade. This unfortunate trend is primed to continue because the aging population is being ravaged by the epidemics of obesity, metabolic syndrome, and diabetes–all of which disproportionately affect women.1) Clearly, this is an important issue. However, misperceptions still exist that cardiovascular disease does not seriously affect women, even though women account for almost 50% of deaths annually.2) Converging evidence from experimental and epidemiological studies indicates that there is an association between chronic psychological distress and cardiovascular disease.3) Many studies have produced evidence to indicate that women report more psychological distress than men.4)5)
The cardiovascular system is thought by many researchers to be the primary target end-organ for the stress response.6) Psychological stress can cause endothelial distress and dysfunction in humans7) and animals.8) Psychological risk factors such as anxiety and depression have been associated with coronary artery disease (CAD). Stress can impact risk factors for CAD such as high blood pressure (BP), physical inactivity, and being overweight. Enhanced sympathetic nerve activity (SNA) plays a major role in the development of atherosclerosis and endothelial dysfunction. Chronic physical pain and mental stress may enhance SNA and alter the function of the sympathetic nervous system (SNS). Disequilibrium of the autonomic nervous system increases SNS activity at rest, along with a deficiency of SNS-mediated responses to certain stimuli such as postural change or exercise.9)
Mindfulness-based stress reduction (MBSR) is a structured group program that employs mindfulness meditation to alleviate suffering associated with physical, psychosomatic, and psychiatric disorders. It was originally developed to manage chronic pain and is now used widely to reduce psychological morbidity associated with chronic illnesses and to treat emotional and behavioral disorders. MBSR may be helpful in controlling several risk factors for coronary heart disease such as hypertension, type 2 diabetes mellitus, dyslipidemia, oxidative and psychosocial stress, obesity, and smoking. MBSR may also improve submaximal exercise responses and heart rate variability (HRV). Although the most effective mode of stress reduction therapy is yet to be established, MBSR therapy is receiving increasing recognition. This study assessed the impact of stress reduction on cardiovascular disease, especially changes in myocardial and endothelial function after MBSR in women.
Methods
Study population
This prospective, observational, single-center cohort study included a total of 34 female patients who were diagnosed with microvascular angina between March 2016 and March 2017. Microvascular angina was defined as typical chest pain with ischemic evidence on ECG or treadmil test and normal coronary angiogram. Exclusion criteria were: any systemic diseases such as significant liver disease, neurologic disorders, or malignancy; secondary hypertension; valvular heart disease; symptomatic arrhythmia and history of heart failure. Demographic characteristics included age, sex, height, weight, and past medical history. Blood was drawn to measure total serum cholesterol, triglycerides, high-density lipoprotein and low-density lipoprotein cholesterol, blood glucose, HbA1c, creatinine, high sensitivity C-reactive protein, free T4, and thyroid stimulating hormone. Body mass index (BMI) was calculated as the ratio of dry weight in kilograms to height in meters squared. Office BP was measured on first admission date. All enrolled patients were treated with conventional anti-anginal agents such as nitrates, calcium channel antagonists, beta-receptor antagonists, and nicorandil during MBSR without regimen changes. Participants were asked to complete the Symptom Checklist 90 Revised (SCL-90-R) survey to assess the grade of mental stress. Myocardial function, endothelial function, and grade of mental stress were assessed both before and after MBSR treatment, and parameters were compared between the two groups. This study was approved by the Institutional Review Board of Kosin University School of Medicine (KUGH 2016-01-023), and all patients were required to provide written informed consent before participation.
Assessment of myocardial function
Two examiners with significant experience in echocardiography and strain analysis performed echocardiography. Standard two-dimensional (2D) strain echocardiography was performed using a 3.5-MHz transducer on the Vivid E-9 Dimension (General Electric, Horten, Norway). 2D grayscale imaging (frame rate ≥ 70/sec) and color Doppler tissue imaging (frame rate ≥ 115/sec) were obtained on apical 2-chamber, 3-chamber, and 4-chamber views using narrow sector angles. Three cycle heartbeats were collected from each view and one selected cycle was analyzed using the Echo PAC Dimension system (General Electric). The global longitudinal strain (GLS) was measured to evaluate global left ventricular (LV) longitudinal myocardial function. GLS follows the endocardial border to the end-systolic frame and uses an automated tracking algorithm to outline the myocardium in consecutive frames throughout the cardiac cycle. Myocardial motion is analyzed by speckle tracking within the region of interest bounded by the endocardium and epicardium. Inappropriate tracked segments are automatically excluded from the analysis, and local strain is calculated for each segment under these conditions.
Assessment of endothelial function
Flow-mediated dilatation (FMD) was performed using 2D ultrasonography (Vivid E-9, General Electronics Corp.) and a modification of the method of Corretti et al.10) Measurements were performed on the subject's left arm after 10 to 20 minutes of rest in the supine position. The brachial artery was longitudinally scanned just above the antecubital crease using an 8.0-MHz linear-array transducer. The diameter of the brachial artery was measured at the R wave of the surface electrocardiogram and at the interface between the tunica media and tunica adventitia of the anterior and posterior walls. Hyperemia was induced by inflation of a pneumatic cuff to 180–200 mm Hg (50 mm Hg higher than systolic BP) for four minutes on the most proximal part of the upper arm. The maximal diameter of the brachial artery was measured 45–60 seconds after sudden deflation of the cuff. The percent brachial artery FMD induced by reactive hyperemia was expressed as the relative change from the baseline [percent FMD = 100 × {(diameter after hyperemia-baseline diameter)/baseline diameter}]. Each diameter was measured three times during two heartbeats, and mean values were used for the final analysis. An independent examiner who was blinded to the study performed the measurements.
Structure and features of MBSR
MBSR is a structured program that runs for 8 weeks with practice once a week (about two and a half hours), education, and one hour of daily practice. It is an education and healing program in which group learning (15–30 persons) is realized through mutual learning, understanding various experiences and the synergy of group dynamics. MBSR consists of mindfulness training, body scan, sitting meditation, and hatha yoga. In addition, daily meditation, yoga, and awareness training are given as homework to enhance the observation ability of participants. Changes in participant status before and after the program are assessed using a variety of measures including depression, anxiety, anger, and global stress index.
Statistical analysis
Statistical analyses were performed with the commercially available computer program SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA). Data were presented as mean ± standard deviation for continuous variables. The Mann-Whitney U test was used for continuous variables. Data normality was tested using the Kolmogorov-Smirnov test. Parameter differences between groups were evaluated using an independent Student's t-test for normally distributed variables or the Kruskal-Wallis test for non-normally distributed variables. Relationships between variables were examined with Pearson correlation coefficients. A two-tailed p < 0.05 was considered statistically significant.
Results
Baseline characteristics
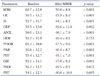
A total of 34 female patients with microvascular angina were analyzed, and their baseline clinical features are shown in Table 1. Mean age was 52.2 years, and global LV systolic function, LV chamber dimension, and LV mass index were normal in all patients with stress. Medical history was consisted of hypertension (n =12, 35.3%), dyslipidemia (n = 6, 17.6%), and diabetes mellitus (n = 7, 20.6%). Most of the patients were under the anti-anginal medications such as calcium channel blocker (n = 25, 57.4%), beta-blocker (n = 15, 44.1%), nitrates (n = 16, 47.1%), and statin (n = 28, 82.4%). None of the medications were permitted to be changed during the study period.
Changes after MBSR treatment
The compliance of this study was approximately 80% in the study group. After 8 weeks of programmed MBSR treatment, most stress parameters (somatization, compulsivity, interpersonal sensitivity, depression, anxiety, phobic anxiety, paranoid ideation, and psychoticism) decreased significantly, except hostility (Table 2). After MBSR treatment, systolic BP was significantly decreased (126.4 ± 16.5 mm Hg vs. 122.2 ± 9.0 mm Hg, p = 0.047), but not the diastolic BP (79.6 ± 12.8 mm Hg vs. 77.2 ± 9.5 mm Hg, p = 0.297). GLS was significantly improved compared to baseline (-19.5 ± 2.1% vs. -16.6 ± 2.5%, p < 0.001) (Table 3). Reactive FMD was also significantly improved (8.9 ± 3.0% vs. 6.9 ± 2.6%, p = 0.005) after MBSR (Table 3). Intra-observer and inter-observer variability for repeated measurements were 0.02 ± 0.05 mm and 0.03 ± 0.18 mm, respectively. Changes in GLS correlated with changes in FMD (r = -0.381, p = 0.034) (Fig. 1). When the correlation between stress parameters and change in myocardial function was assessed, changes in GLS correlated with changes in stress parameters [Global Severity Index (GSI), r = 0.295, p = 0.015; obsessive compulsivity, r = 0.259, p = 0.033; interpersonal sensitivity, r = 0.256, p = 0.035; depression, r = 0.311, p = 0.010; anxiety, r = 0.352, p = 0.003; hostility, r = 0.240, p = 0.049; phobic anxiety, r = 0.264, p = 0.030; paranoid ideation, r = 0.258, p = 0.034; Positive Symptom Distress Index, r = 0.374, p = 0.002].
We also divided the study group as responders and non-responders for MBSR according to the improvement of GSI (responder; improvement of GLS ≥ 10%, non-responder; improvement of GSI < 10%) and analyzed the change of GLS and FMD. Responder group showed significant improvement of GLS change than non-responder group (-3.55 ± 2.96% vs. -1.59 ± 2.54%, p = 0.008). But there was no significant difference of FMD change between the groups (2.52 ± 3.07% vs. 1.25 ± 4.61%, p = 0.247) (Fig. 2).
Discussion
This study identified several important findings. First, MBSR significantly reduced stress parameters. Second, after MBSR, myocardial function and endothelial function significantly improved. Third, changes in GLS were proportionally correlated with changes in stress parameters.
Stress and heart
The link between psychosocial factors such as stress and CAD has drawn significant attention. Chronic stressful stimuli such as work stress, marital stress, caregiver strain, low social support, and low socioeconomic status have been linked to increased risk of CAD and other adverse cardiac events.11) There is also evidence that emotional stressors can act as triggers for acute cardiovascular events.12) We previously demonstrated that myocardial longitudinal deformation and endothelial function are reduced in patients with chronic emotional stress, as assessed by 2D strain echocardiography and brachial FMD.13) Recently, in a multicenter prospective cross-sectional survey of 163 Korean women with chest pain, the presence of depression was evaluated using the Beck Depression Inventory and Lee and Rhee Depression scales.14) This study demonstrated that depression is associated with a prolonged corrected QT interval, CAD, and coronary vasospasm in female patients with chest pain, suggesting a possible mechanism by which depressive mood may be linked to coronary endothelial dysfunction and atherosclerosis. These results suggest a mediating role of emotional regulation in the development of depression and physical illness.
MBSR, cardiovascular disease, and stress reduction
Mindfulness is defined as the capacity to intentionally be in the present moment without judgment.15) This approach assumes that greater awareness provides more veridical perception, reduces negative affect, and improves vitality and coping. MBSR is based upon a systematic procedure to develop enhanced awareness of moment-to-moment experience of perceptible mental processes.16)17)18) The mechanism of healing consists of the following elements: relaxation, become insensitive, acceptance, self-control, and flexibility. The MBSR program is an oriental psychological practice method introduced to the medical field by Kabat-Zinn15) at the University of Massachusetts. Since then, MBSR has been investigated as a new treatment for diverse chronic diseases and anxiety, depression, and other psychological disorders. Meditation mediates physiological changes by inducing relaxation of the parasympathetic nerves that have a potent reaction to stress caused by excitation of the SNS. During the practice of meditation, brain waves refer to the most awakened cognitive state. During meditation, there are abundant theta waves, which are reported to increase not only cognitive function but also physical performance capacity. A study on the impact of MBSR on improving well-being (i.e. relaxation states and related positive emotions) in a sample of 42 physicians for a period of one year (8 week MBSR program with an additional 10 month maintenance period) showed significant improvements in the experimental group compared with the control group regarding levels of mindfulness and relaxation.19)
The present study showed that MBSR has beneficial impacts on myocardial function in female patients with microvascular angina. There are various mechanisms that improve cardiac function with MBSR. Depression and rumination impair the ability to process negative information, and hypothalamic pituitary adrenal axis over-activation is associated with higher rates of cortisol production. MBSR enhanced quality of life, decreased stress symptoms, and altered cortisol and immune patterns are consistent with less stress and mood disturbances.20) MBSR reduces symptoms of anxiety, depression, and perceived stress, which also contributes to lowered BP and improved cardiac function. Nyklíček et al.21) showed that MBSR decreased overall systolic and diastolic BP compared to the control group and controlling for age, sex, BMI, and beta-blockers from pre- to post-intervention. In our study, also we observed that systolic BP was decreased after MBSR with the controlled medication. Another study showed that patients of the MBSR group had therapeutic gains such as lowered BP.22) When the correlation between stress parameters and changes in myocardial function was considered, changes in GLS were closely associated with changes in most stress parameters. This result supports a direct link between the degree of stress reduction and improvement in myocardial function.
There is some evidence that MBSR improves autonomic balance. MBSR decreased heart rate, an effect that was maintained a year after beginning treatment.23) Nijjar et al.24) also showed that participation in an 8 week MBSR program improved frequency domain parameters of HRV during meditation, suggesting improved sympatho-vagal balance. MBSR reduced sympathetic and increased parasympathetic influences compared to controlled respiration alone, suggesting that MBSR could be a useful adjunct in the management of conditions with reduced HRV, such as acute myocardial infarction and heart failure.25)
Because chronic stress induces vascular stiffness, MBSR also has a beneficial impact on vascular function. We previously identified that chronic pain exerts a negative effect on endothelial function in patients with fibromyalgia, and reduced endothelial function was associated with an increased risk of vascular stiffness in patients with fibromyalgia.26)27) MBSR had beneficial effects on reducing vascular stiffness, shown by reduced basal SNS activity. In our study, MBSR improved pre- to post-intervention endothelial function as assessed by reactive FMD in female patients with microvascular angina.
Our study has several limitations. First, our study has no control group. To avoid additional impacts of drug on improving LV function and endothelial function, we tried to control anginal medication during MBSR intervention. Second, the number of enrolled patients was too small to generalize results. Finally, we did not analyze male patients in the MBSR group, as the effects of MBSR on men and women may differ. There are some reports of gender differences in MBSR. Female patients with coronary heart disease showed significant differences in breathing patterns, physical functioning, and submaximal exercise responses during exercise following the 8 week MBSR program without differences in resting levels of stress hormones.28) Another study showed that female participants exhibited a significantly larger decrease in diastolic BP during meditation, whereas men had greater increases in cardiac output during meditation. These results indicate both similarities and differences in physiological responses to body scan meditation and other relaxing activities.29) Because the effects of MBSR are thought to be greater in women than in men, we decided to conduct the study only on women.
It is difficult to explain the exact mechanisms of the effects of psychological factors on cardiac function. Understanding the factors that govern the variety of health outcomes that different people experience following exposure to stress has important implications for the development of effective emotion-regulation interventional approaches (e.g., mindfulness-based therapy, emotion-focused therapy, and emotion regulation therapy).30) More experimental rather than conceptual evidence is needed to practice and understand this concept.31)
Conclusion
MBSR is not only useful in reducing psychological stress, but also in improving LV function and endothelial function. Although the most effective mode of stress reduction therapy is yet to be established, increasing recognition is being given to MBSR therapy, especially in women who are susceptible to stress.




 XML Download
XML Download