

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Stress-induced cardiomyopathy (SCMP) is characterized by transient systolic dysfunction of the left ventricle (LV) without significant coronary artery stenosis1) and is closely associated with acute emotional or physical stress.2) The clinical features are similar to acute myocardial infarction: typical chest pain, electrocardiographic changes, wall motion abnormalities on echocardiography, and elevation of cardiac biomarkers. The prognosis of SCMP is generally thought of as favorable,3) but the clinical progress can be fatal depending on the severity of the underlying systemic illness, according to recent reports.4)5)
SCMP is reported to be more common in women than men, especially postmenopausal women.6)7)8)9)10) Less is known about differences in clinical characteristics of female and male patients with SCMP, with some evidence that male patients have a lower incidence and poor prognosis.11)12)
Accordingly, the objectives of this study were to compare clinical characteristics and prognosis between female and male SCMP patients and to investigate whether gender is associated with mortality and major cardiac complications.
Methods
Study design and patients
We reviewed electronic medical records of patients clinically suspected to have SCMP at our hospital. Prospectively recruited patients from January 1997 to December 2005 were included from a previous report,13) and the remaining patients were retrospectively collected from January 2006 to August 2014. The Institutional Review Board Committee of our institution approved the study protocol (IRB No. 2015-12-016).
SCMP was diagnosed based on criteria for Takotsubo syndrome from the Mayo Clinic, Rochester, MN, USA.3) Type of SCMP was determined by LV morphology on 2D echocardiography. Typical apical type was characterized by transient apical hypokinesis with basal hyperkinesis of LV myocardium. Non-apical type was determined when the myocardium showed hyperdynamic apex with akinetic base movement; or akinesis of midventricular segment with hyperdynamic base and apex.14)15)16)
Data collection
Demographic and clinical data included age at diagnosis, sex, cardiovascular risk factors, preceding stress events, initial presentation, and chest X-ray (CXR), along with electrocardiographic and echocardiographic data. Preceding stress events were classified as emotional or physical. Physical stressors were classified as post-operative, other acute medical illness, or trauma.
Laboratory data included complete blood count, electrolytes, lipid profiles, and inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein, as well as cardiac biomarkers such as creatine kinase MB, troponin-I, and N-terminal prohormone of brain natriuretic peptide (NT-pro BNP). ST-segment elevation was defined as new-onset ST elevation more than 1 mm measured 80 milliseconds after the J point in more than 2 contiguous leads, and T-wave inversion was defined as negative T waves more than 3 mm in amplitude in more than 2 contiguous leads.17) Left ventricular function and wall motion abnormalities were assessed from the modified Simpson's method using two-dimensional transthoracic echocardiography.18) In all patients, absence of coronary thrombosis or angiographic evidence of acute plaque rupture was confirmed with coronary angiography within 48 hours of onset. Diagnosis of pulmonary edema was made on the CXR.
The severity of systemic illness at the time of diagnosis was semi-quantified by the Acute Physiology and Chronic Health Evaluation (APACHE) II scoring system.19) In-hospital management included: 1) intubation/mechanical ventilation, 2) use of a mechanical supporter such as intra-aortic balloon pump, extracorporeal membrane oxygenation, 3) use of inotropes, and 4) heart failure medication: angiotensin-converting-enzyme inhibitor/angiotensin receptor blocker (ACEi/ARB) and/or beta-blocker.
Outcomes
Outcome parameters were defined as all-cause mortality and major cardiac complications. Major adverse cardiac and cerebrovascular events (MACCE) were defined as cardiac death, recurrence of SCMP, ischemic heart disease, major arrhythmias, and stroke. Major arrhythmias included sustained ventricular tachycardia (VT), ventricular fibrillation, and advanced atrioventricular block that required medical treatment or permanent pacemaker/implantable cardioverter defibrillator (PPM/ICD) implantation.
Statistical analysis
Categorical variables are presented as frequencies and percentages. The chi-square test or Fisher's exact test was performed as appropriate to test differences of categorical variables between the two groups. Continuous variables are presented as mean ± standard deviation. Student's t-test was performed to test differences of continuous variables between the two groups. Receiver operating characteristic curves were calculated to evaluate the use of APACHE II score as a prognostic indicator of mortality. The probability of freedom-from-death and freedom-from-MACCE were estimated according to the Kaplan-Meier method and log-rank test. p values < 0.05 were considered significant. Multiple Cox proportional hazard regression analysis was performed to determine clinical correlates of all-cause mortality and major cardiac events. We considered collinearity between each parameter above and APACHE II score, so that these parameters were not included in the multiple analysis together with APACHE II score to avoid collinearity problems.20) Data ware analyzed using SPSS statistical software (version 20.0 for Windows, IBM Corp., Armonk, NY, USA).
Results
Study population and baseline characteristics
There were 54 patients enrolled in a prospective study between January 1997 and December 2005.13) From January 2006 to August 2014, 266 patients were clinically suspected to have SCMP and global wall motion abnormalities in the mid-ventricle or apex on echocardiography. Among them, 49 patients who had no significant coronary artery disease on urgent coronary angiography and no evidence of myocarditis were retrospectively included. Ultimately, a total of 103 patients were included in this study, with a median age of 65 years (range, 28 to 87 years); male patients accounted for 31.9% of the total (70 female vs. 33 male). Median follow-up duration was 25.6 months (range 2 to 194.7 months). Baseline clinical characteristics, laboratory findings, echocardiographic findings, and clinical outcomes according to sex are presented in Table 1.
Gender differences in baseline clinical characteristics and antecedent stressor
There were no differences between men and women in age (63.2 ± 12.2 vs. 61.3 ± 15.7, female vs. male; p = 0.501), history of malignancy (p = 0.117), underlying chronic organ failure (p = 0.057), or cardiovascular risk factors, except for history of smoking, which was significantly more common in male patients (p < 0.001).
There were also no statistical differences regarding symptoms between groups, though chest pain was more likely to be present in female patients [33 (47%) vs. 9 (27.3%); p = 0.057]. White blood cell count was higher in men compared with women (p = 0.001), which corresponded with a higher proportion of acute medical illness in men, otherwise no difference was demonstrated regarding cardiac markers, NT-pro BNP or other laboratory results. Mean APACHE II score at the time of SCMP diagnosis was similar in males and females (13.6 ± 5.7 vs. 13.2 ± 7.7, p = 0.752). ECG findings were also similar. There was no significant difference between two groups on the in-hospital use of ACEi/ARB or beta-blocker.
Pump failure at initial echocardiography was more severe in male patients [ejection fraction (EF): 34.6 ± 9.3% vs. 39.8 ± 11.3%, respectively; p = 0.024]. The mean left ventricular ejection fraction (LVEF) at follow-up within two months was still lower in male than in female patients (50.3 ± 12.5% vs. 57.0 ± 11.7%; p = 0.022). Most patients showed complete recovery of LVEF (n = 76, 73.8%) without gender difference, but seven patients (6.8%) failed to recover at all during the follow-up period. There was no difference in ballooning type between men and women (p = 0.828).
Most patients (86.4%) had a preceding stress event, caused by physical stress in 67 (65.0%) and emotional stress in 16 (15.5%). Physical stressors were more commonly present in male than in female patients [27 (81.8%) vs. 40 (57.1%), respectively; p = 0.014], whereas emotional stressors were present mostly in female patients [15 (21.4%) vs. 1 (3.0%), respectively; p = 0.016]. Acute medical illness was the only physical stressor that was statistically different between the two groups [18 (54.5%) vs. 22 (31.4%), male vs. female; p = 0.025].
Clinical outcomes
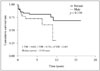
During the follow-up period, all-cause mortality was observed in 22 patients (21.4%). The most common cause of death was related to malignancy (n = 13, 59.1%). Cardiac death occurred in 3 patients (2.9%): 1 died during a hospital stay due to severe heart failure and VT, 1 died after recurrence of SCMP and 1 died because of sudden cardiac death. MACCE were observed in 22 patients (21.4%): congestive heart failure in 14, recurrence of SCMP in 9, major arrhythmia in 7, and stroke in 4. Overall cumulative survival was 84.2, 78.1, and 60.1% at 1, 5, and 10 years, respectively. Kaplan-Meier survival curves did not reveal statistical differences between sexes (p = 0.220) (Fig. 1). Likewise, Kaplan-Meier event-free survival curves were not statistically different (67.8% vs. 73.9%, male vs. female; p = 0.942).
MACCE were observed in 23 patients (22.3%) including recurrence of SCMP in 9 patients (2 patients recurred twice: one occurred stroke simultaneously and the other one died of cardiac arrest), major arrhythmia requiring medical treatment or PPM/ICD insertion in 7 patients, stroke in 4 patients, ischemic heart disease in 1 patient, and cardiac death in 3 patents. Event-free survival was 79.2, 72.6, and 62.2% at 1, 5, and 10 years, respectively.
Predictors of all-cause mortality and MACCE
Preceding physical stress and reduced LVEF at follow-up after 2 months were significant independent risk factors for all-cause mortality on Cox proportional hazards regression analysis. In the subgroup analysis of males, reduced follow-up LVEF after 2 months [hazard ratio (HR): 0.89, 95% confidence interval (CI): 0.82–0.95; p = 0.001] was an independent risk factor of all-cause mortality. Meanwhile, APACHE II score ≥ 15 (HR: 5.27, 95% CI: 1.07–25.9; p = 0.041) was an independent risk factor of all-cause mortality in females (Table 2).
In addition, univariate and multiple analysis were performed to determine clinical correlates of major cardiac and cerebrovascular complications. Age ≥ 65 and pulmonary edema on initial CXR were demonstrated to be risk factors of MACCE in univariate analysis, but not in the multiple analysis. LVEF ≥ 58% on follow-up echocardiography (HR 0.24, 95% CI 0.09–0.66; p = 0.006) was demonstrated to be significant risk factors of MACCE in patients with SCMP in univariate and multiple analysis.
Discussion
The present study investigated gender differences in clinical profiles of patients with SCMP. Male patients accounted for 31.9% of total study patients, which is similar to previous reports (range 21–37%) of SCMP in Korean populations,19)21)22) but significantly higher than in studies of non-Asian populations where about 10% (range 0–18%) of the study patients are men.11)12)23) These findings suggest ethnic differences in clinical profiles of SCMP.
Overall cumulative survival was not statistically different between male and female patients, in contrast to previous reports of male sex as a predictive risk factor. Brinjikji et al.12) found that in-hospital mortality of males was 2.5 times higher than that of females. In that study, male SCMP patients had a higher incidence of underlying critical illnesses than females. Conversely, Kurisu et al.11) found no significant difference in inhospital mortality between males and females, despite a higher incidence of in-hospital onset of SCMP in male patients.
Underlying malignancy and lower LV systolic function after 2 months were independent predictors for all-cause mortality. LVEF after 2 months appeared to be a significant prognostic determinant of both of all-cause mortality and MACCE during the long-term follow-up period. These findings are similar to previous studies of clinical correlates of SCMP.242526)
Antecedent stress factors affected clinical outcomes. Women with a physical stressor as a trigger had a higher risk of all-cause mortality than those with an emotional stressor. Moreover, the clinical progress of women was different depending on APACHE II score, which reflects the severity of the preceding physical stressor. Few studies have specifically investigated antecedent stress as a prognostic factor of SCMP. In a recent study, Núñez-Gil et al.27) reported that physical stress as a trigger of SCMP was associated with poor prognosis. However in that study, more than 90 percent of the patients were women, making it difficult to apply the result to the general population. Further studies are warranted to better understand gender differences in the prognostic influence of antecedent stressors. We suggest that lower survival in women with preceding physical stress might be driven by a higher APACHE II score, since APACHE II score is a significant predictor of in-hospital mortality.21)22)
Meanwhile, male patients without complete recovery of LV systolic dysfunction after 2 months had a higher risk of all-cause mortality than the others. We suggest that pump failure in men is more profound and takes longer to recover from, which could affect clinical outcomes.
Study limitations
As our study is partially retrospective, serial follow-up of echocardiography and laboratory test were not performed in all patients. In addition, we included patients diagnosed with definite SCMP, which could be both a limitation and strength of this study. All patients underwent coronary angiography to rule out significant coronary disease, which suggests that selection bias could exist. On the other hand, this study could be interpreted to have a verified outcome of subjects with definite diagnosis compared to other studies. Finally, a relatively small number of patients had clinical events in the current study, resulting in limited study power to find statistically significant clinical correlates of deaths or cardiac complications.
Conclusion
This report identified gender differences in clinical profiles in a Korean population. First, SCMP was more common in female patients. Second, the clinical characteristics of SCMP were similar between men and women, with the exception of more severe LV systolic dysfunction in men. Third, antecedent emotional stress was more common in female patients, whereas physical stress was more common in male patients. Finally, inhospital clinical course and long-term clinical outcome appeared to be similar between men and women. In predicting clinical outcome, preceding physical stress and lower LV systolic function after 2 months were associated with poor clinical outcomes in both genders. In addition, women with severe physical illness and men with severe systolic dysfunction after 2 months had a greater risk of poor prognosis than the others.


 XML Download
XML Download