

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Vasovagal syncope (VVS) is the most common cause of postural syncope, and has a lifetime cumulative prevalence of 35%.1) The vasovagal decrease in heart rate or blood pressure (BP) usually leads to an increase in the reflex sympathetic stimulation of the ventricular myocardium, which in turn causes the activation of the ventricular vagal afferent C-fiber connecting to medullary vasomotor centers. The head-up tilt test (HUTT) is widely recognized as an effective technique for providing evidence of susceptibility to neurally-mediated syncope.2) Although the precise etiology and pathophysiological events underlying VVS are not fully understood,3) there is consensus that the autonomic nervous system is the final common pathway leading to syncope. Therefore, cardiovascular autonomic modulation may play a role in the occurrence of syncope in patients with HUTT-induced VVS.4)5)
Recently, there has been a great deal of interest on the potential role of epicardial adipose tissue (EAT) as a cardiovascular risk factor. Epicardial fat represents the visceral fat depot of the heart displaying high metabolic activity.6) A high amount of epicardial fat tissue has the capacity to produce several mediators with unique endocrine and paracrine functions that affect the cardiac autonomic system.6)7)8) Thus, we can hypothesize that cardiac autonomic function could explain the connection between epicardial fat thickness (EFT) and VVS. However, no previous studies have examined the association between HUTT-induced VVS and EFT as measured by echocardiography.
Therefore, the purpose of this study was to investigate the association between EFT and the HUTT in patients undergoing HUTT for the evaluation of unexplained syncope. Based on the key role of the autonomic nervous system in VVS, we hypothesized that increased EFT would reflect autonomic abnormalities that would help distinguish individuals with positive HUTT results from those with negative HUTT results.
Methods
Study population
This is retrospective, single-center study included a total of 855 patients with syncope or near syncope between March 2006 and June 2015, all patients underwent HUTT and echocardiography. Inclusion criteria were as follows: 18–70 years of age, normal renal function, and for women, a regular menstrual cycle. Exclusion criteria were: any systemic diseases such as significant liver disease, neurologic disorders or malignancy; secondary hypertension; valvular heart disease; symptomatic arrhythmia; a positive treadmill test; a history of heart failure; a history of acute coronary syndrome; a history of myocardial infarction or any revascularization procedure. And we also excluded all type 2 diabetes mellitus patients to avoid effect of diabetes in autonomic cardiac modulation and VVS. Demographic characteristics recorded at the first visit included age, sex, height, weight, current medications, smoking history and past medical history. Blood was drawn for the measurement of total serum cholesterol, triglycerides, high-density lipoprotein (HDL) and low-density lipoprotein cholesterol, blood glucose, creatinine, uric acid, and high sensitivity C-reactive protein. Body mass index (BMI) was calculated as the ratio of dry weight in kilograms to height squared (in square meters). This study was approved by the institutional review board. All patients were required to provide written informed consent to participate.
Head-up tilt table test
The HUTT was performed after overnight fasting and during sinus rhythm, usually between 8:00 am and 12:00 pm. All cardioactive and vasoactive drugs were withdrawn at least 7 days before. Informed consent was obtained from all participants. The patient was stabilized in the supine position for 5 min and tilted at 60° for 20 min to induce syncope. If syncope was not induced, the patient was given 2.5 mg of sublingual nitroglycerin spray at a 60° tilt. Twelve-lead ECG tracings and BP were measured every 2.5 min throughout the HUTT. If syncope or hypotension (systolic BP < 80 mm Hg) occurred, the patient was moved into the Trendelenburg position and the test was promptly terminated. A positive response to the HUTT indicated the development of syncope or presyncope in association with hypotension, bradycardia, or both. We divided the patients into two groups based on HUTT results (positive vs. negative). The patients who experienced syncope during the test were divided into three groups based on the presence of bradycardia, hypotension, or both during the onset of syncope. A vasodepressor response was defined as a decrease in systolic BP to < 60 mm Hg without a decrease in heart rate during symptoms. A cardio-inhibitory response was defined as an abrupt decrease in heart rate by ≥ 20% without any antecedent decrease in systolic BP. A mixed response was defined as a concurrent decrease in systolic BP to < 60 mm Hg and a decrease in heart rate by ≥ 20% compared to these values 4 min before the onset of symptoms.
Echocardiographic measurement
We performed echocardiogram all of the patients to differentiate the structural heart disease causing syncope such as aortic stenosis, hypertrophic cardiomyopathy, left ventricular outflow tract obstruction. Echocardiogram was performed immediately before HUTT. Standard 2-dimensional echocardiography was performed on all participants while lying in the left lateral decubitus position using a 3.5-MHz transducer (Philips iE33, Philips Medical Systems, Bothell, WA, USA). The echocardiographers were blinded to patient information. Measurements of the thickness of the interventricular septum and posterior wall, the diameter of the left ventricle (LV) cavity, and the LV mass index were performed according to the criteria outlined by the American Society of Echocardiography.9) Echocardiographic assessments of EFT, defined as the echo-free space between the outer wall of the myocardium and the visceral layer of the pericardium, were measured perpendicularly from the free wall of the right ventricle at end-systole in three cardiac cycles according to the method we previously described.10) Because one critical issue in EFT measurement is inconsistency of measurement location, the mean EFT was averaged from images from the parasternal long axis, parasternal short axis and apical 4-chamber view. The intra- and inter-observer variability of the EFT was 3.3% and 5.8%, respectively.
Statistical analysis
Statistical analyses were performed with the commercially available computer program SPSS 18.0 for Windows (IBM Corp., Armonk, NY, USA). Data were presented as mean ± standard deviation for continuous variables and their percentages (%) for categorical data. The Mann-Whitney U test was used for continuous variables and the chi-square test was used for categorical data. The normality of the data was tested using the Kolmogorov-Smirnov test. Parameter differences between groups were evaluated using an independent Student's t-test for normally distributed variables or the Kruskal-Wallis test for non-normally distributed variables. Relationships between variables were examined with Pearson correlation coefficients. The cutoff value of EFT for predicting a positive HUTT with corresponding sensitivity and specificity was estimated by receiving operator characteristic (ROC) curve analysis. Multivariate logistic regression models for a positive HUTT were built to determine which variables were independently associated with this status. A two-tailed p < 0.05 was considered statistically significant.
Results
Comparison of clinical characteristics and hemodynamic types of syncope
A total of 797 consecutive patients (mean age 46.5 years, male: 45.7%) were analyzed and their clinical features according to HUTT result are shown in Table 1. There were 329 patients (41.3%) with negative HUTT results and 468 patients (58.7%) with positive HUTT results. There were no differences between subjects with positive and negative HUTT results with respect to age and heart rate (Table 1). However, HUTT-positive patients were more likely to be female and have a significantly lower waist circumference, BMI, and systolic and diastolic BPs. When analyzing only male patients, both waist circumference and BMI was lower in HUTT-positive patients and higher EFT than HUTT-negative group (Supplementary Table 1). When analyzing only female patients, there was no significant difference of waist circumference and BMI between groups (Supplementary Table 2). According to the hemodynamic responses accompanying the syncope, 468 HUTT-positive participants were classified as follows: 62 vasodepressive responses, 107 cardio-inhibitory responses, and 299 mixed responses.
Comparison of echocardiographic parameters
There were no significant differences in cardiac chamber size between groups with the exception of the left atrium, ejection fraction, and mitral inflow patterns (Table 2).
However, EFT was significantly higher in HUTT-positive patients compared to HUTT-negative patients (HUTT-positive, 5.69 ± 1.76 mm vs. HUTT-negative, 5.24 ± 1.60 mm; p < 0.001) (Fig. 1A). Furthermore, we estimated EFT values among the three hemodynamic types of syncope, and found that there were no significant differences among the groups with respect to EFT (vasodepressive responses, 5.6 ± 1.5 mm; cardio-inhibitory response, 5.8 ± 1.9 mm; and mixed responses, 5.7 ± 1.8 mm; p = 0.669) (Fig. 1B).
Correlations between EFT and VVS
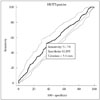
On the ROC analysis, EFT > 5.4 mm was associated with a positive HUTT result with 51.7% sensitivity and 63.8% specificity [area under curve: 0.578, 95% confidence interval (CI) = 0.54–0.61, p < 0.001] (Fig. 2). Univariate logistic regression analysis showed that a positive response was associated with female sex, left atrial diameter, HDL cholesterol, waist circumference, systolic BP and EFT [hazard ratio (HR): 1.02, 95% CI: 1.01–1.03, p < 0.001]. Furthermore, multivariate logistic regression analysis revealed that EFT (HR: 1.02, 95% CI: 1.01–1.03, p = 0.004) was an independent predictor of a positive HUTT result (Table 3) after adjusting for variables with significant univariate impact. When we performed subgroup analysis for the multivariate regression according to the use or non-use of medications, in particular beta blockers, the results did not differ.
Discussion
To the best of our knowledge, this is the first study investigating the association between EFT and HUTT. The most relevant findings obtained from this study are as follows: 1) epicardial fat was thicker in patients with a positive HUTT result, 2) multiple logistic regression analyses showed that an increased EFT was an independent predictor of positive HUTT in patients with unexplained syncope. Our findings suggest a possible link between epicardial fat and autonomic dysregulation in HUTT-positive VVS.
Although VVS is a common clinical event, its pathophysiological mechanism has not yet been fully elucidated. The syncopal symptoms of VVS appear to be associated with pathological autonomic cardiac modulation.11)12) The neurally-mediated syncopal syndromes encompass a number of apparently related disturbances of reflex cardiovascular control characterized by transient inappropriate bradycardia and/or vasodilation of various arterial and venous beds. VVS results from simultaneous enhancement of parasympathetic nervous system (vagal) tone and abrupt withdrawal of sympathetic nervous system tone.13)14)15)16) In addition, it was postulated that there is a ‘ mismatch' between the neural signal to the skeletal muscle vasculature and the release or availability of noradrenaline.17) One previous study showed that an imbalance in myocardial autonomic nerve function plays an important role in inducing VVS.4) HUTT is a wellvalidated and effective technique for the evaluation of vasovagal reactions, which may be responsible for syncopal episodes.18) Thus, it is conceivable that patients with HUTT-positive VVS present with abnormalities of autonomic circulatory control.
Increased plasma fatty acid levels may stimulate the cardiac autonomic nervous system through an increase in plasma catecholamine concentrations. EAT is anatomic storage of fat with endocrine, paracrine, and vasocrine effects on the myocardium. 19) These effects are due to the lack of a fibrous fascial layer impeding diffusion of free fatty acids and adipokines between the tissue and the underlying vessel wall and myocardium.20)21) Moreover, EAT contains abundant ganglionic plexi, which interact with the extrinsic sympathetic and parasympathetic nervous system to modulate the cardiac autonomic system.22)23) Thus, patients with a large amount of EAT may have increased intrinsic adrenergic and cholinergic nerves.20) A recent study showed that altered sympathovagal balance, as detected by disturbed heart rate variability and heart rate turbulence, was observed in patients with higher EAT thickness, and this influence was independently correlated with EAT thickness.24) Interestingly, in our study, HUTT-positive group showed lower BMI and waist circumstance than HUTT-negative group. Although epicardial fat is known to be associated with metabolic syndrome, hypervagotonic activity is more likely to be affected in patients with VVS. There may be possible mechanism that people who are obese of having high body mass can respond and adapt better to situation of fainting of vasovagal event than thin people. There have been approved that a low weight and low BMI has been found to be a risk factor of VVS during transfusion.25) So we think EAT is not simple reflecting parameter of visceral fat. It may have own pathophysiology and element to affects vagal activity.
Consequently, there may be a possible correlation between EFT as assessed by echocardiography and HUTT-positivity in patients with neurally-mediated syncope. The principal finding of our study is that patients with VVS with a positive tilt test also had increased EFT. In addition, there was a significant and independent interaction between EFT and HUTT-positivity, which can be explained by the fact that the EAT contains rich ganglionic plexi that have both adrenergic and cholinergic nerves. Interestingly, the increase in the EFT was not dependent upon the hemodynamic type of syncope. To the best of our knowledge, this is the first study to evaluate the relationship between EFT as an indicator of autonomic nervous system disturbances and a positive HUTT result in patients with VVS. Although this conclusion cannot be drawn with certainty, we speculate that the discordance between the autonomic nervous system and increased intrinsic cardiac autonomic tone may lead to a deterioration of baroreceptor-cardiac reflex sensitivity in subjects with greater EAT thickness.
Consequently, there may be a possible correlation between EFT as assessed by echocardiography and HUTT-positivity in patients with neurally-mediated syncope. The principal finding of our study is that patients with VVS with a positive tilt test also had increased EFT. In addition, there was a significant and independent interaction between EFT and HUTT-positivity, which can be explained by the fact that the EAT contains rich ganglionic plexi that have both adrenergic and cholinergic nerves. Interestingly, the increase in the EFT was not dependent upon the hemodynamic type of syncope. To the best of our knowledge, this is the first study to evaluate the relationship between EFT as an indicator of autonomic nervous system disturbances and a positive HUTT result in patients with VVS. Although this conclusion cannot be drawn with certainty, we speculate that the discordance between the autonomic nervous system and increased intrinsic cardiac autonomic tone may lead to a deterioration of baroreceptor-cardiac reflex sensitivity in subjects with greater EAT thickness.
Our study has several limitations. First, to decrease the effect of ischemic symptoms after the termination of the exercise test, we excluded patients with a history of heart failure, revascularization, or a positive result on an exercise test. However, the presence of coronary artery disease was excluded using only exercise testing, and further stress imaging modalities were not used. Second, this study is retrospective and was performed at a single tertiary care center, it is possible that there were biases with respect to patient referral and population sampling. Third, the correlation power between EFT and HUTT result was weak. Forth, we didn't analyzed linear correlations between EFT and changes of BP or HR during HUTT. But when we estimated EFT values among the three hemodynamic types of syncope, there were no significant differences among the groups with respect to EFT. Finally, EFT can be affected by metabolic syndrome, raising the possibility of an association between metabolic syndrome and EFT.
In conclusion, EFT, an indicator of cardiac autonomic activity, was increased in patients with HUTT-positive VVS, in whom abnormal parasympathetic reactivation occurs. EFT was an independent predictor of a positive HUTT. Our findings suggest a possible link between epicardial fat and autonomic dysregulation in HUTT-positive patients with VVS. The association between EFT and adverse cardiovascular outcomes in HUTTpositive patients with VVS needs to be investigated in further detail through future research.




 XML Download
XML Download