

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Treatment of end-stage left ventricular (LV) heart failure (HF) is a constantly updating health issue. Although a fundamental resource, heart transplantation remains a limited tool, widely insufficient to satisfy the demand of refractory HF patients treatment. LV assist devices (LVAD) have been progressively shifting from bridge to transplantation therapy alone to an increasing use as destination therapy for not suitable for transplantation-patients.1)2) Even if this fact represents a thrilling advancement in HF treatment, it opens the question of suitability to LVAD implantation. In fact, failing hearts may vary widely even at end-stage disease. Current data on morbidity and mortality in patients underwent to LVAD implantation confirm such assumption.3)
More specifically, a focus on right ventricle needs to be open. Right ventricular (RV) systolic function has a strong ability to stratify prognosis in patients with HF and a coexistent RV dysfunction is associated with poorer exercise capacity and reduced survival in these patients.4)5)6)7)8)9) RV systolic function is the best recognized factor on whom the outcome of LVAD patients depends.10)11)12)13) Nonetheless, according to different definitions, 6–44% of patients undergo RV failure after LVAD surgery.14)15) The Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) defines RV failure as need of an RV assist device (RVAD) or requirement of inhaled nitric oxide or inotropic therapy for > 1 week any time after LVAD implantation in the presence of symptoms and signs of persistent RV dysfunction, such as central venous pressure > 18 mm Hg with a cardiac index < 2.3 L/min per square meter in the absence of elevated left atrial or pulmonary capillary wedge pressure (> 18 mm Hg), cardiac tamponade, ventricular arrhythmias, or pneumothorax.1) It is therefore crucial to evaluate RV morphology and, above all, function prior to confirm the eligibility of any patients to LVAD. It appears, however, equally important to monitor the right ventricle during the last days before device implantation, in order to minimize both long-term and short-term RV dysfunction. Transthoracic echocardiography is a reliable, versatile and bedside-available tool for this kind of evaluation.
Factors determining RV output and function include RV preload, afterload, and contractility. Implant of LVADs inevitably affects all such factors, possibly leading to acute RV dysfunction. RV preload increases as a result of increased cardiac index–which can augment up to 100%.16) In addition, perioperative period constitutes an adjunctive stress since a substantial amount of fluids and blood products are often administered to patients. This acute increase in preload leads to overstretching of cardiac myofibrils beyond the point of optimal contractility based on Frank-Starling principle, and thus to decreased RV stroke volume. Furthermore, increase in RV preload may lead to RV annular dilatation and tricuspid regurgitation, adding further load to RV demand. Since RV function and, secondly, structure in HF patients is strictly dependent on the effect of LV dysfunction itself,17) a consistent number of patients with terminal LV dysfunction unfortunately have coexistent at least initial RV dysfunction. Fleeting or weak right ventricles may not tolerate the new hemodynamic equilibrium following LVAD implantation and, consequently, fail.
In recent years, many studies have tried to find predictors or to develop models and scores aimed to foretell RV failure risk after LVAD implantation.11)12)18)19)20)21)22)23)24)25)26)27)28)29)30)31)32) A plethora of clinical, laboratory, hemodynamic, and echocardiographic variables have been found to be associated with RV failure or need of RVAD implantation. Cardiac index, RV stroke work index (RVSWI), vasopressor requirement, serum creatinine, bilirubin or aspartate aminotransferase, blood pressure, preoperative low pulmonary arterial pressure, tricuspid incompetence, RV short/long axis ratio, tricuspid annular motion, and RV longitudinal strain (RVLS) are just some examples. It is evident how poor accordance exist in this field, not only about which variables are linked to RV failure, but also about a more basic point: the focus on RV response capability towards increased preload, increased cardiac output and continuous aortic flow that follow LVAD implantation. There is a strong rationale for considering RV contractility as the key point.
The aim of such models is to exclude the eligibility to LVAD through an accurate patients selection. The matter is not to identify overt biventricular failure but to intercept those patients with slight, initial, subclinical RV dysfunction who are particularly likely to develop frank RV failure after LVAD, thus encountering a poorer prognosis. This knowledge may pave the way to further development of differentiated standardized protocols of peri-operatory management for patients at major risk of RV failure after surgery, which may be a far better solution rather than pre-operative or, even worst, post-operative shift to biventricular assist device. Transthoracic echocardiography provides the most reliable and, very importantly, soon and easily repeatable parameters for RV evaluation, allowing a tight follow-up in perioperative period as well as on long-term period.
Physicians' attention should be shifted from “what to do if RV failure occurs after LVAD implantation” to “how can we avoid RV failure to occur after LVAD implantation.” Aim of this paper is to provide a concise review of RV echocardiographic indexes of function in the setting of assessing patients eligibility to LVAD implantation, and to propose a protocol to be standardized as a routine tool in patients evaluation in order to reduce morbidity and mortality among these patients.
Echocardiographic Parameters
Despite RV ultrasound imaging has been challenging and, as a consequence, neglected for a long time, there are several parameters which reliably describe RV morphology and function.
Tricuspid annular plane systolic excursion
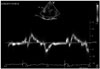
Normal RV function is highly dependent on longitudinal shortening. Tricuspid annular plane systolic excursion (TAPSE) measured through M-mode is a widely used index of RV function (Fig. 1). In the initial validation study, TAPSE correlated strongly with radionuclide angiography, with low interobserver variability.33) Nevertheless, TAPSE is a regional, linear parameter for a complex structure and is dependent on loading conditions and insonation angle. Therefore, it is not uncommon to under- or over-estimate RV systolic function according to TAPSE, especially in failing hearts. In a study of 750 patients with a variety of cardiac conditions, TAPSE yielded high specificity but low sensitivity to distinguish abnormal from normal subjects.34) Although TAPSE has been reported to predict RV failure,23) further studies in LVAD patients did not confirm this finding.35)36)37)
Systolic velocity with tissue Doppler imaging
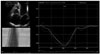
Tissue Doppler imaging (TDI) is an attractive alternative to TAPSE because myocardial velocities are easy to obtain and reproduce (Fig. 2). Systolic velocity (S') of the tricuspid annulus reflects longitudinal RV function. However, velocities depend on insonation angle and loading conditions. Also, translational motion of the heart and tethering by adjacent diseased myocardial segments can produce velocities that are not representative of the performance of the interrogated segment. In a study of 68 recipients with LVAD, systolic tricuspid annular velocity did not predict RV failure.38)
RV longitudinal strain
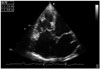
Among imaging techniques, speckle tracking echocardiography (STE) has recently been applied to the study of RV function. It allows an objective and quantitative evaluation of global and regional myocardial function, independent of the angle of insonation and from cardiac translational movements (Fig. 3).39)
In a retrospective study of 117 patients undergoing LVAD implantation, free-wall RVLS by velocity vector imaging predicted RV failure with 76% specificity and 68% sensitivity at a cutoff of -9.6%.10) In another study of 68 patients undergoing elective LVAD surgery, RVLS by speckle tracking was significantly impaired preoperatively (-12.6 ± 3.3% vs. -16.2 ± 4.3%; p < 0.001) in 24 patients (35.3%) who experienced RV failure by 14 days.38)
In other studies, it has been demonstrated that in patients with advanced systolic HF referred for heart transplantation, STE analysis of RV deformation correlates well with RVSWI, an invasive measurement of RV systolic function, providing a better estimation of RV systolic performance than other traditional parameters.30)35) In particular, close negative correlations between global RVLS and free-wall RVLS with the RVSWI were found (r = -0.75 and -0.82, respectively; both p < 0.0001).35) Furthermore, free-wall RVLS demonstrated the highest diagnostic accuracy [area under the receiver operating characteristic curve (AUC): 0.90] and good sensitivity and specificity of 92% and 86%, respectively, to predict depressed RVSWI using a cutoff value of less than -11.8%.35) In the same study, tricuspid S' on TDI and TAPSE were not significantly correlated with RVSWI (r = 0.14 and 0.06; respectively).
Moreover, it has been demonstrated that a low free-wall RVLS has the highest predictive value for post-operatory RV failure in accordance with poor RVSWI in patients underwent to LVAD implantation (AUC: 0.93).40) Finally, in a recent perspective study on 98 patients with systolic HF referred for heart transplantation, during a mean follow-up of 1.5 ± 0.9 years, free-wall RVLS and global RVLS were independently predictive (both p < 0.0001) of combined outcomes of cardiovascular death, hospitalization for acute HF, heart transplantation, intra-aortic balloon pump implantation, and ventricular assist device implantation.41) The overall performance for the prediction of cardiovascular events was greatest for free-wall RVLS (AUC: free-wall RVLS: 0.87; global RVLS: 0.67).
RV fractional area change
RV fractional area change (RVFAC) is a feasible, quantitative technique which allows to estimate RV systolic function. Defined as (end-diastolic area - end-systolic area) / end-diastolic area × 100, it is a measure of RV systolic function which has been shown to correlate with RV ejection fraction (RVEF) by magnetic resonance imaging (MRI).42)43) In the above mentioned study, RVFAC was independently predictive of combined cardiovascular outcomes (cardiovascular death, hospitalization for acute HF, heart transplantation, intra-aortic balloon pump implantation and ventricular assist device implantation) in advanced HF patients referred for heart transplantation (p < 0.0001; AUC: 0.60).41) In a retrospective study of patients implanted with LVAD, RVFAC was significantly lower in the group of patients who experienced RV failure than in the group without RV failure (24% vs. 30%; p = 0.04).36) However, RVFAC did not predict RV failure in another larger study.44) Technical issues make this index less reproducible than RVLS, such as heavy RV trabeculation and pacemaker or defibrillator-related artifacts in patients with advanced HF. In one study, a > 10% reduction in RVFAC at 1 month was associated with worse quality of life and poor exercise capacity in patients with an LVAD.45)
RVEF with three-dimensional echocardiography
RVEF is a powerful index of RV systolic performance and is generally calculated through cardiac MRI.46) Despite that, many end-stage HF patients are still foreclosed to MRI, being receivers of implanted cardioverter defibrillator or cardiac resynchronization therapy (CRT) devices, that might not be MRI compatible. Three-dimensional (3D) echocardiography has been extensively validated against cardiac MRI.47)48) 3D-echocardiography has become widespread and relatively easy to use. Recently, it has been proposed as an effective alternative to MRI for RVEF calculation in patients with LV dysfunction,49) allowing to overcome technical issues on MRI and providing reliable and objective measurement of RV systolic function. Growing experience and technology development have allowed the comparison of 3D-derived RV volumes and EF with other echo and MRI well established functional parameters.50)51) Specifically, it is notable to underline that ultimate software releases for the analysis of RV function have allowed to significantly ameliorate feasibility and reproducibility since a higher level of semi-automaticity has been introduced.50) Nonetheless, ECG-gated MRI might be limited for RVEF evaluation in patients with significant variability of cardiac cycles duration, such as in atrial fibrillation which is highly prevalent in end-stage HF patients: single-beat 3D-echocardiography might allow to overcome such question.52) Recently, Nagata et al.53) found that RVEF assessed through 3D-echocardiography was independently associated with cardiac outcomes in patients with diverse backgrounds, after determination of methodology accuracy against MRI. For all these reasons, we believe that 3D echocardiography is already a valuable tool for functional evaluation of the right ventricle.
RV index of myocardial performance
RV index of myocardial performance (RIMP) is a functional global index of both systolic and diastolic RV function. It is calculated as the ratio of the isovolumic contraction and relaxation times to the ejection time. A higher ratio means that a large proportion of each cardiac cycle is spent increasing and decreasing pressure without performing stroke work, indicating a worse ventricular performance.54) In patients with advanced HF selected to receive CRT, abnormal RIMP demonstrated to be associated with adverse outcome compared to normal RIMP (0.83 vs. 0.69, p = 0.004) and each 0.1 unit increase in RIMP was associated with a 16% increased risk (95% confidence interval: 8–26).55) Analogous association was also found in patients with moderate chronic HF.56)
RV sphericity index
The RV response to chronic volume and/or pressure overload is dilation. Dilation means a loss of triangular shape in a two-dimensional 4-chamber view imaging, and a tendency towards sphericization. Minor dimensions–i.e., basal and mid diameters–of the right ventricle progressively increase, whereas longitudinal dimension is generally poorly modified (Fig. 4).57) RV sphericity index (RVSI), expressed as the ratio between RV midventricular and longitudinal diameters, is an indicator of RV remodeling that has recently been studied in patients with LV HF. In a cohort of 62 LV HF patients with increased pulmonary arterial hypertension, an increase in RVSI in one-year follow-up predicted clinical deterioration with good sensitivity and specificity (respectively, 70% and 62%, AUC: 0.649).58) RVSI was also increased in a cohort of patients undergoing heart transplant for end-stage HF.59)
The need of systematic RV function analysis: the purpose of SIENA protocol
Echocardiography provides a potentially complete evaluation of RV function in the setting of advanced HF. The echocardiographic indices used in this context are resumed in Table 1, with possible benefits and disadvantages in clinical usage for each of them.
Since RV failure can complicate LVAD implantation, pre-surgery RV analysis should be performed systematically in order to minimize morbidity and mortality of patients treated with LVAD. A systematic pre-operative RV study should be aimed at stratifying the risk of RV post-operative dysfunction. For this aim we will to propose the SIENA protocol, an echocardiographic scoring system, in order to emphasize the need of a systematic ultrasound evaluation of RV function prior to LVAD surgery.
In this review of echocardiographic parameters of RV function, free-wall RVLS, RVFAC, RVEF with 3D-echocardiography and RVSI have emerged as the most promising or best predictive indexes of RV dysfunction after LVAD implantation.
These indices were therefore introduced in our model for the prediction of post-LVAD RV failure. Table 2 summarizes their reference values and our proposal of a systematic protocol that should eventually be investigated in a multicenter, longitudinal study. Fig. 5 supplies a visual abstract of the SIENA protocol.
As a provisional analysis, based on single studies analyzing the single parameters for that aim, a high level of specificity for these parameters appears clear. Waiting a longitudinal study, we propose to give one point for each positive parameter and to identify a higher risk of RV failure for patients with more than one (SIENA score > 1). Subsequently, if data are confirmed, we could use this score as an additional tool to identify patients at higher risk that would be worth of a more intensive evaluation and management.
Conclusion
RV failure after LVAD implantation still remains a huge unsolved problem and constitutes an unacceptable source of morbidity and mortality. Time has come to find an accordance about risk stratification in pre-operatory evaluation of patients undergoing LVAD. Assessment of RV capability to react to the new hemodynamic setting due to LVAD is a key point, and transthoracic echocardiography provides the best indexes of RV function. We think that RV evaluation in LVAD-candidate patients should be a routine analysis in every center. In particular, we propose the Systematic LVAD Implant Eligibility Non-invasive Assessment protocol, the SIENA protocol, to be studied as a routine program of suitability evaluation before LVAD implantation focused on RV pre-operatory function. Such protocol would be part of a more global clinical evaluation of patients, being based on transthoracic echocardiographic variables which include: free-wall RVLS, RVFAC, RVSI, and RVEF with 3D-echocardiography. Feasibility, quick availability and reproducibility appear as the highlights of this protocol. A multicenter prospective study needs to be performed in order to eventually establish its potentially powerful role.




 XML Download
XML Download