

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Echocardiography has become an integral diagnostic tool in a clinical field of cardiology.1) Progress of acoustic and digital image processing technology has made echocardiography readily available, convenient, inexpensive, and time-saving diagnostic modality, whereas inherent disadvantages of cardiac ultrasound still exist.2)3)4) Endocardial border delineation (EBD) is important to evaluate left ventricular (LV) volume and ejection fraction (EF). Especially patients with obesity, lung disease, mechanical ventilation, surgical drains and tubes may have a poor echo window.5)6)7)8) LV volume and EF were consistently underestimated by baseline echocardiography than cardiac magnetic resonance image.9)10) Low level of confidence with suboptimal echocardiography leads to repetitive test or other types of diagnostic examination, causing increased patient's medical cost and healthcare system burden.11)12)13) About 15% of routine echocardiogram and up to 30% of echocardiogram in critically ill patients are suboptimal.14) Highly subjective and examiner dependent feature is another pitfalls of echocardiogram without contrast. Inter-observer and intra-observer variability of non-contrast echocardiography (CE) have been under criticism.
CE uses high molecular weight microbubble enclosed by lipids, albumin, or surfactant.15)16) Very low mechanical index (MI) ultrasound has enabled more pronounced nonlinear echo signal from microbubble while suppressing linear echo signal from myocardium.15)16) Clear left ventricular opacification (LVO) and EBD can be acquired by using ultrasound contrast agents (UCAs) in patients with poor image on harmonic echocardiography. CE boasts 95% of EBD and conversion of 75% of previously non-diagnostic, poor echo results to interpretable ones.17) Trainee or novice in echo labs get the benefit more than expert from CE in not-echo-friendly circumstance as intensive care unit (ICU).18)19) Impact of CE on clinical decision making was reported in US20) and impact of CE in ICU patients also reported in Korea.21) We examined impact of CE on assessment of LV function and diagnosis in routine clinical echocardiography in Korea.
Methods
Patient selection
From March, 2008 to March, 2011, 260 patients were prospectively enrolled at 12 Korean teaching hospitals. Following routine rest echocardiography, discretionary CE was performed on same patients. The study was approved by Institutional Review Committees at each hospital. A total of 12 expert physicians were involved in care of patients who enrolled. Myocardial CE and stress echocardiography were excluded.
Echocardiography protocols with and without contrast
Two-dimensional and spectral Doppler echocardiography were recorded from apical and parasternal windows. Second harmonic imaging and high MI (1.0 to 1.5) were used to acquire echocardiography without contrast. When routine echocardiogram was deemed suboptimal to interpret, Definity (Lantheus Medical Imaging, North Billerica, MA, USA) or SonoVue (Bracco Diagnostics, Milan, Italy) were delivered by bolus injection or by continuous infusion and MI was adjusted to low level (0.3 to 0.5). Both images were stored digitally and interpreted within several hours.
Investigation of echocardiogram
Two independent observers participated. Conventional echocardiography was interpreted by one observer and then CE image was interpreted by the same observer. Another observer evaluated full echocardiographic results with and without contrast at once. Target variables were: global image quality, visualized LV segments, LV apex, LV EF, right ventricle (RV). Semi-quantitative grading was used to categorical variables.
Evaluation of the clinical impact
After baseline echocardiography is done, attending physician was contacted and has answered further diagnostic and management plan. CE result was exposed to the same physician, and he or she was questioned about possible changes of diagnostic and treatment plan.
Assessment of safety
Within 24 h after UCAs injection, any of all following: death, cardiac arrest, myocardial infarction, arrhythmia requiring immediate intervention, anaphylactoid reaction, or hypotension were regarded safety end points.
Statistical analysis
SPSS for Windows (version 12.0; SSPS Inc., Chicago, IL, USA) was used for statistical analysis. Study population statistics were presented as mean ± SD for continuous variables and count percentages for categorical variables. McNemar test was used to reveal significant proportional differences between two groups. Wilcoxon signed rank test was used to compare the number of visualized LV segments before and after contrast. A p value of 0.05 or lower was considered to be statistically significant.
Results
Patients and echocardiography characteristics
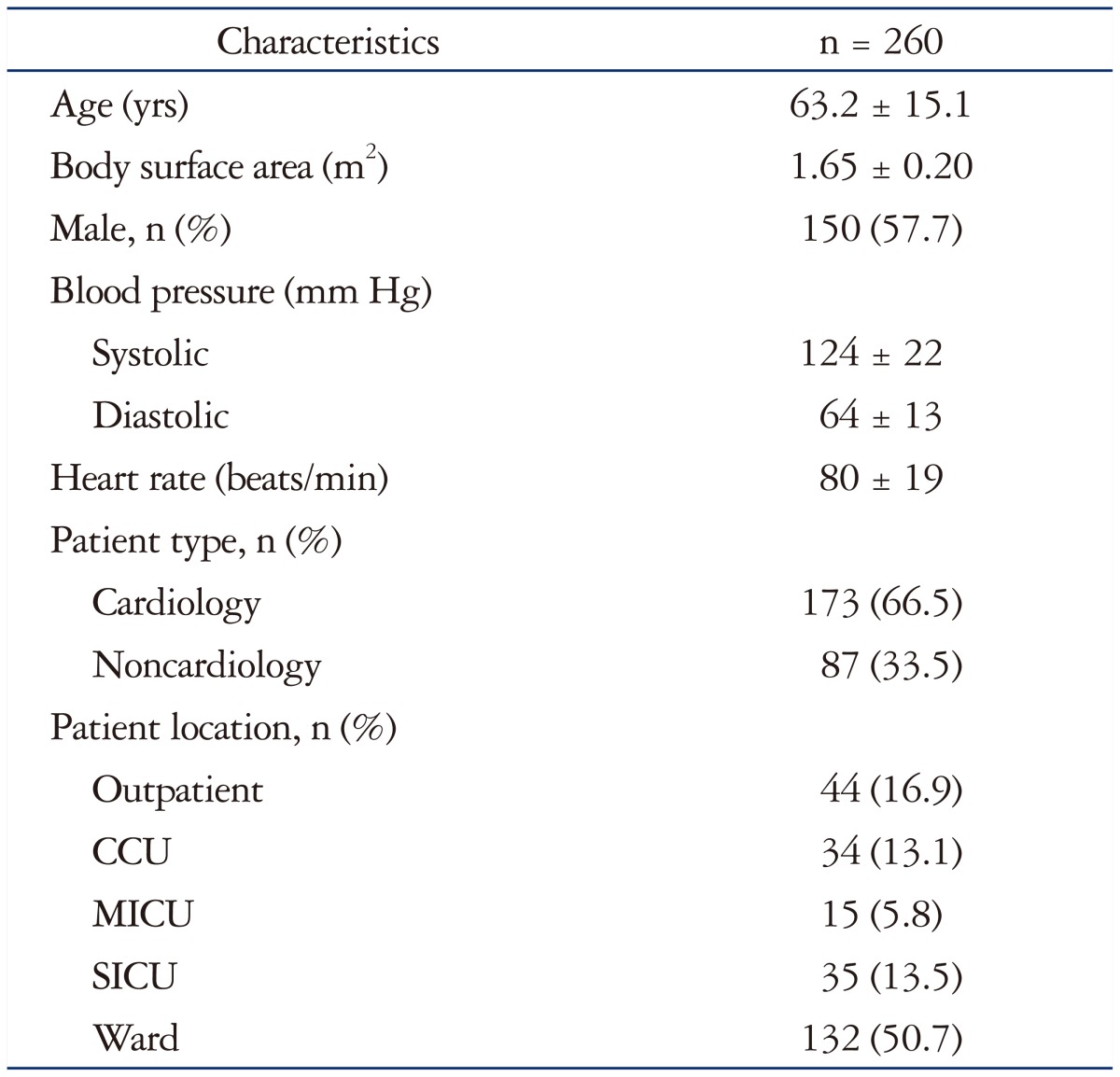
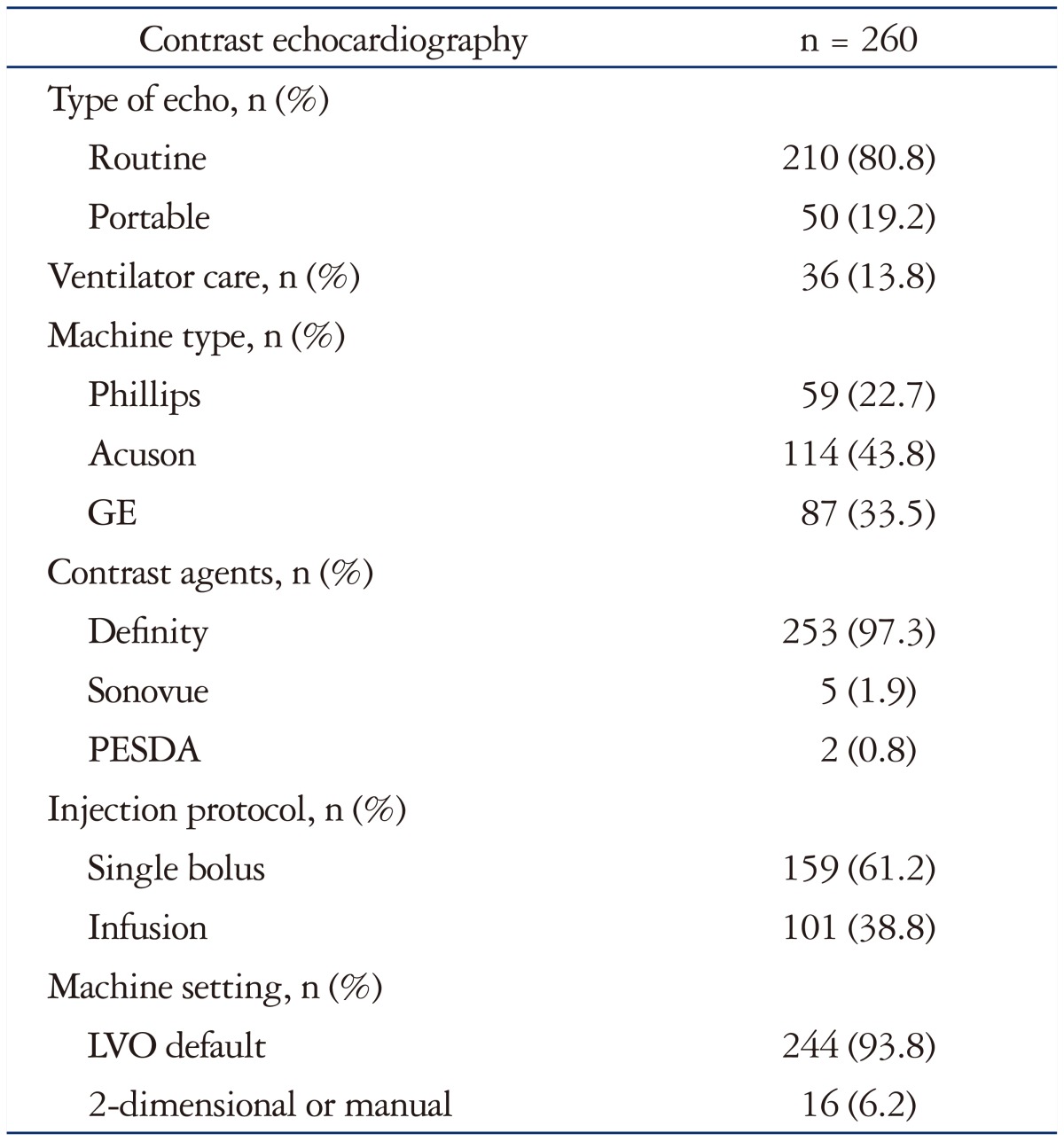
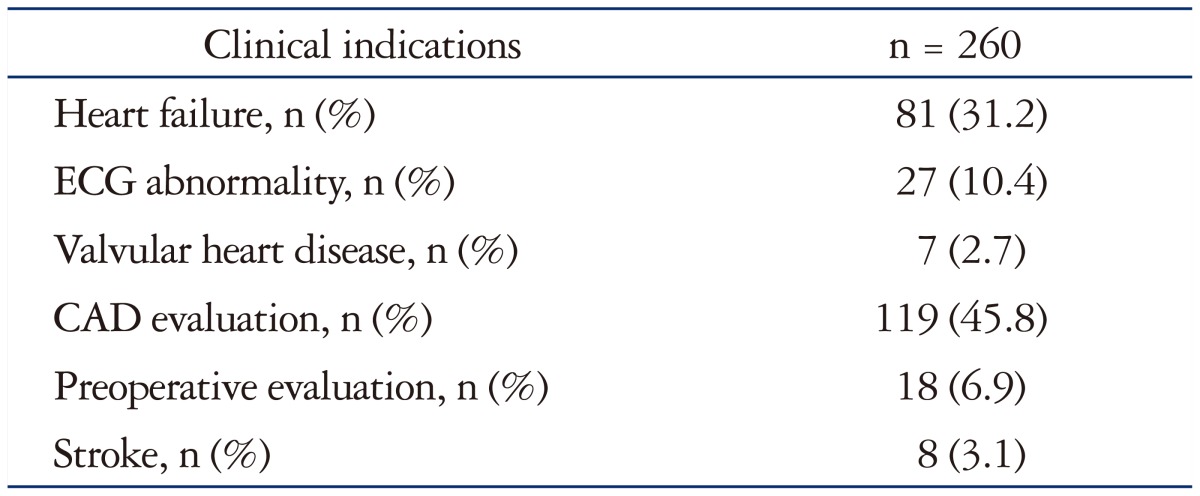
A total of 260 patients with routine or portable echocardiography who underwent CE were enrolled. Baseline patient characteristics are listed in Table 1. Mean age was 63.2 ± 15.1, male patients were 57.7%, cardiology patients were 66.5%, outpatients were 16.9%, and patients in any kinds of ICU were 32.4%. Table 2 shows baseline echocardiographic characteristics. Routine echocardiography was 80.8% of all test, portable echocardiography was remaining 19.2%. Patients with mechanical ventilator were 13.8%. Echocardiography vendors were Acuson (43.8%), GE (33.5%), and Philips (22.7%). UCAs used in study were mostly Definity (97.3%). Microbubble contrast was bolus injected (61.2%) or continuously infused (38.8%). Heart failure (31.2%) and coronary artery disease (45.8%) were main reasons for echocardiography (Table 3).
Benefits of CE
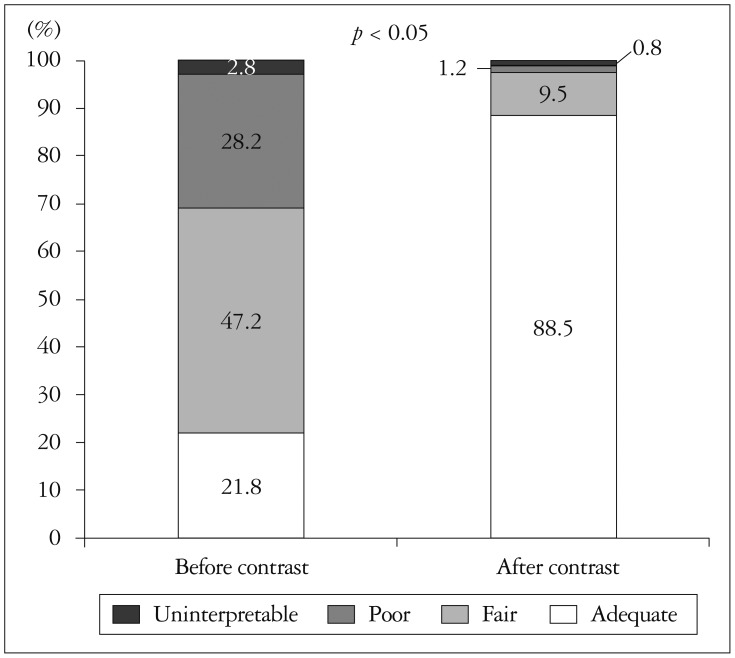
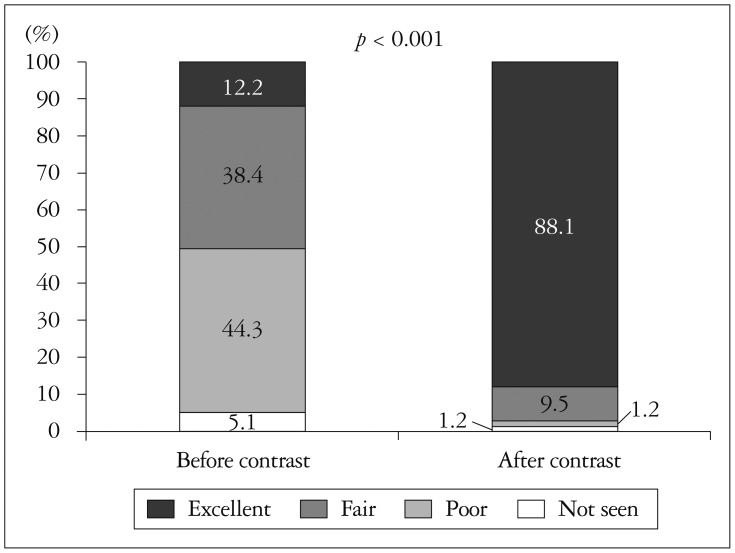
General image quality was classified under four headings; adequate (full endocardial visualization), fair (greater than 50% visualized endocardium), poor (minimal endocardial visualization), or uninterpretable (only epicardium visualized). Before contrast delivery, poor or uninterpretable echocardiography comprised 31% which decreased to 2% after contrast delivery (Fig. 1). The number of visualized LV segments per person was 9.53 before contrast, which increased significantly to 14.46 after contrast (p<0.001). The percentages of inadequate assessment of LV wall motion, before and after contrast, were 28.4% and 3.5%, respectively (p<0.001). LV apex delineation was also greatly increased by contrast. Baseline echocardiography has resulted in 49.4% of unsatisfactory echo views to rule out LV thrombus confidently. CE revealed LV apex more clearly, only 2.4% of all subject was ambiguous (Fig. 2). In patients whose LV EF was calculated, CE made a small but significant increase of EF; from 48.38% to 49.62% (p<0.05). The percentage of poor or not seen RV from apical view were 30.5% without contrast, 10.5% with contrast (p<0.001).
Clinical impact of CE
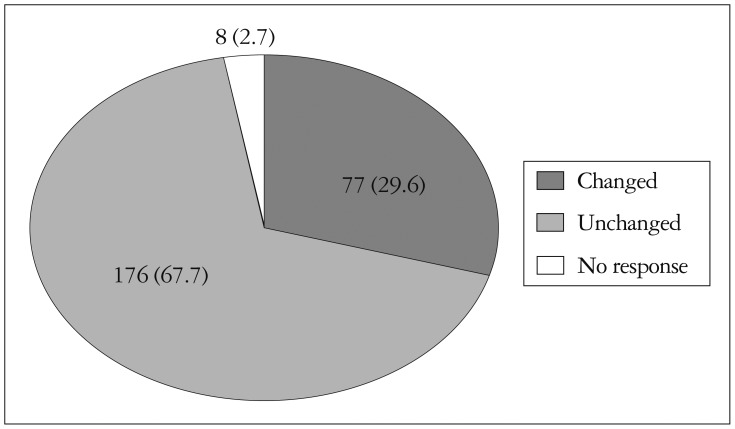
CE influenced clinical diagnostic and drug management plan. Thirty percent of all CE result has made changes of further diagnostic procedure (i.e., cancelling nuclear imaging, transesophageal echocardiography, or diagnostic angiography). Treatment plan was also changed by physicians after CE review, 29.6% of all subjects (Fig. 3).
Discussion
This Korean multicenter study showed that CE augmented general image quality, confidence, global and regional LV function assessment, RV image quality and influenced physician's diagnostic and management plan. Suboptimal echo images with routine and portable echocardiography necessitate other expensive medical modalities.2)3)4) CE-LVO produces clearer EBD than fundamental echocardiography, especially in patients with obesity, chronic obstructive lung disease, altered mentality who are difficult to image.1)22)23)24) Commercially available contrasts have prolonged time span of opacification and high blood to myocardium signal ratio.25) UCAs are hemodynamically inert and have a same rheology as blood cells.26)27) In addition, CE is useful in stress echocardiography,28) LV thrombus or mass detection,29) RV and great vessel examination,30)31) mitral regurgitation and aortic stenosis grading.32)33)
Large multicenter prospective clinical trial in US was reported in 2009 by Kurt et al.20) A total of 632 patients with technically difficult images were enrolled. Baseline patient characteristics in US study and in this Korean study are almost same except mean body surface area (BSA). An average BSA in US study was 2.09 m2, whereas an average BSA in Korean study was 1.65 m2. In general image quality, 11.7% of patients were uninterpretable in US study, but 2.8% of patients were uninterpretable in Korean study. This disparity is a possible consequence of higher body mass or BSA in US patients. Echo windows in Korean patients are slightly better than in US patients. CE revealed more endocardial segments assessment than fundamental echocardiography consistently in both studies; 5.3 more visualized segments after contrast in US, 4.9 more visualized segments after contrast in Korea.
Cohen et al.17) reported superiority of CE for LV EBD in 203 patients with suboptimal echo images in a US prospective multicenter trial. Kitzman et al.22) showed improvement of EBD with CE in 211 patients with suspected cardiac disease and suboptimal fundamental echocardiograms in a US multicenter study. In a European multicenter trial, 100 patients planned for routine coronary angiography with or without heart failure were enrolled.34) CE increased inter-observer agreement of regional wall motion. A total of 218 patients with suspected coronary heart disease were enrolled in a European multicenter study by Senior et al.35) CE was safe and effective for LV EBD. Hwang et al.21) reported impact of contrast agent on assessment of LV function and on clinical diagnosis in a Korean prospective multicenter trial on ICU patients. Our study included not only selective population enrolled by previous studies but also routine clinical population. Therefore, this study might reflect well benefit of CE in real clinical practice.
This study has some limitations. First, cost-effectiveness of CE was not fully and specifically calculated with health insurance reimbursement data. Second, the study was not fully blinded by physicians and sonographers. Pre-expectation of observers may cause biased results. Automated assessment function by vendors was not used in EF estimation or wall motion analysis to reduce human errors. Third, readers, observers, and cardiologists in 12 teaching hospitals did not have same exact echocardiographic measurement technique, experience in cardiac echo labs, clinical decision making standards. Lastly, relatively small sample size.
However, this study is a first Korean multicenter study that investigated the utility of CE in a routine clinical echocardiography. And it showed CE was still useful despite Korean patients had relatively low BSA. Also, this study suggested the efficacy of CE in real routine clinical world because study population included not only patients in ICU or with poor echo window but also patients in routine clinical echocardiography environment.
In conclusion, regarding routine clinical echocardiography in Korean population, CE in comparison with fundamental echocardiography improved LV function assessment and clinical decision making.
 XML Download
XML Download