

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Unicuspid aortic valve (UAV) is an extremely rare form of congenital aortic valvular abnormality. UAV shows similar clinical characteristics to bicuspid aortic valve (BAV), except the clinical symptoms develop at earlier age and progress at a faster pace in UAV.1) UAV was first reported in 1958 by Edwards,2) and its prevalence is about 0.02% in the general population based on having echocardiographic examinations.3) However, the incidence of UAV has been reported as approximately 4–6% of the patients who underwent aortic valve (AV) replacement.4)5)
UAV has been categorized into 2 subtypes: pin-hole shaped acommissural UAV and slit-shaped unicommissural UAV. Pin-hole-shaped acommissural UAV is usually accompanied by severe aortic stenosis, and its symptoms occur in infancy. The later type of UAV has a relatively larger valve area, and symptoms present later in the forth to sixth decades of life.1)6)
In this report, we are presenting a case of severe aortic stenosis associated with unicommissural UAV. The patient underwent a successful Bentall operation. Although we have only one reported case of an asymptomatic UAV in Korea,7) this case had significant symptoms associated with severe aortic stenosis, and unicommissural UAV was confirmed in the surgical specimen.
Case
A 42-year-old man was referred to our cardiovascular clinic for the recent worsening of exertional dyspnea and chest discomfort that had started 12 months previously. He reported no symptoms at rest but had a feeling of tightness and bursting-like pain in the chest when walking fast or going uphill in the past year. The patient was told that he had congenital heart disease in childhood. However, he was unsure of the exact diagnosis and had not been receiving follow-up care. He had no family history of sudden cardiac death or cardiac disease and reported no current medication or surgical history.
At the time of his presentation, his vital signs were: blood pressure, 120/80 mm Hg; respiratory rate, 18 breaths/min; heart rate, 82 beats/min; body temperature, 37℃; and oxygen saturation, 98% (room air). In physical examinations, grade 4/6 systolic ejection murmur was heard at the right upper sternal border. The electrocardiogram showed normal sinus rhythm and severe left ventricular (LV) hypertrophy with a strain pattern. There was no cardiomegaly or other specific finding on chest radiograph.
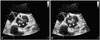
Transthoracic echocardiography revealed marked LV hypertrophy with normal LV systolic function. The AV was thickened and heavily calcified in the middle portion. There was a fissure-like opening in the anterior side of the AV suggesting unicommissural UAV (Fig. 1, Supplementary movie 1). The measured AV area by 2-dimensional plannimetry was 0.70 cm2, and there was no aortic regurgitation. The maximal velocity through the AV was 6.0 m/sec, mean pressure gradient between the aorta and the AV was 94 mm Hg, and the calculated AV area was 0.66 cm2. The ascending aorta showed a fusiform dilation up to 50 mm.
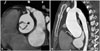
Because the patient was diagnosed with severe aortic stenosis associated with UAV, we performed a computerized tomographic (CT) scan to demonstrate the anatomy of the aorta and exclude the presence of other combined congenital anomalies including coarctation of the aorta. The CT scan of the aorta revealed a thickened and heavily calcified UAV with aneurysmal dilation of the ascending aorta (Fig. 2, Supplementary movie 2). There was no evidence of a stenotic portion or calcified plaque in the coronary artery and no specific findings suggesting coarctation of the aorta.
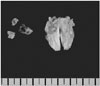
The attending physician recommended surgical treatment of the symptomatic severe aortic stenosis with post-stenotic aneurysmal dilation of the ascending aorta. The patient was referred to another hospital for surgery and underwent a Bentall procedure. The surgical specimen clearly showed a unicommissural UAV with severe calcification (Fig. 3). The patient was discharged without complications after surgery.
Discussion
In this report, we present a case of severe aortic stenosis associated with unicommissural UAV.
UAV is a rarely reported congenital heart disease. Normally, the AV develops with 3 cusps formed from 3 tubercles during cardiogenesis.8) However, a UAV develops when the 3 cusps are fused or failed to separate.9)
Because patients with a pinhole-shaped acommissural UAV are detected in their infancy, adult patients with UAV will have a unicommissural UAV. Adult patients with a UAV share many clinical features with patients with a BAV, including valvular dysfunction, aortic dilation, aortic dissection, and dysmorphic calcification.1)9) However, UAV patients generally show symptoms more earlier in their lives, usually in 30–50 years, and valvular dysfunction develops earlier and progresses at a faster pace in UAV patients than in aortic stenosis patients associated with a normal tricuspid AV.1)9)10) One reported study showed that a smaller number of aortic cusps was associated with a greater incidence of valvular dysfunction or degeneration of the ascending aorta.11)
Echocardiography is the best imaging tool in the detection of a UAV because it can evaluate the valve morphology, valve orifice, annular attachment zone, and the severity of aortic stenosis or regurgitation. It can also obtain information about the ascending aorta, LV change due to hemodynamic load, and associated congenital deformities including patent ductus arteriosus and aortic coarctation. However, given that the prevalence of an UAV is about 0.02% in the adult population, the actual incidence identified by the using echocardiography as a pre-operative diagnostic tool seems to be an underestimate. Of the 231 cases in a systematic review in 2010, only 10% were diagnosed before surgery,1) and Noly et al.12) showed that only 14% of UAV was diagnosed by the preoperative echocardiography. Other diagnostic tools for an UAV include cardiac CT or cardiac magnetic resonance imaging. Because these modalities became sensitive to detect AV structure with technical progression, the preoperative detection of a UAV can be increased with these imaging studies.
Severe aortic stenosis or mixed stenosis and regurgitation are common forms of valvular dysfunction in UAV. Like BAV, UAV can be also accompanied by aortic dilatation or aortic dissection. If the aortic root or ascending aorta is involved, surgical treatment is usually required. A recent study reported that UAV was specifically accompanied by dilatation at the aortic annulus level,12) and our patient also showed dilatation, with the ascending aorta of 50 mm and the aortic annulus of 32 mm.
In conclusion, we report a case of UAV presenting in the form of severe aortic stenosis, in which the diagnosis was eventually confirmed in the pathologic specimen after the surgery.
 XML Download
XML Download