

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Diastolic dysfunction is known to develop after myocardial damage.1)2) Deceleration time (DT) and mitral E wave to flow propagation velocity ratio are examples shown to be associated with adverse remodeling and/or poor prognosis after acute myocardial infarction (AMI).3)4) While systolic dyssynchrony was well studied and found to be associated with adverse remodeling in patients with AMI, little attention has been paid to diastolic dyssynchrony (DD) in those patients.5)6) This study was conducted to investigate the incidence of DD during acute ST segment elevation myocardial infarction (STEMI) and its impact on functional recovery of left ventricle (LV) thereafter.
Methods
Patients
The study was designed as a longitudinal observational study. Consecutive patients who presented with first acute STEMI within 12 hours of symptom onset and treated with primary percutaneous coronary intervention were prospectively enrolled. Additionally, a control group from outpatients with similar demographic characteristics but without known coronary artery disease or heart failure was included for comparison. Patients who presented after 12 hours of symptom onset or patients in whom successful revascularization could not be achieved were not included. Patients with wide QRS complexes (> 120 ms) in baseline electrocardiography were excluded as systolic and DD were already described in those patients.7) All patients gave written informed consent and the study was approved by Local Ethics Committee.
Echocardiography
First echocardiographic examination was performed within 48 hours of admission. Echocardiographic images were acquired with a commercial ultrasound system (Vivid 5, General Electric Vingmed, Horten, Norway) using a 2.5–3.5 MHz phased array probe with standard harmonic imaging in left lateral decubitus position. LV end-diastolic volume (EDV), end-systolic volume (ESV), and ejection fraction (EF) were calculated from apical 2- and 4-chamber views using modified Simpson's method. Left atrial volume (LAV) was calculated from apical 2- and 4-chamber views using area length method. EDV, ESV, and LAV were indexed to body surface area for uniformity [EDV index (EDVI), ESV index (ESVI), and LAV index (LAVI), respectively]. Standard diastolic filling parameters such as mitral inflow E and A waves, E wave DT, isovolumic relaxation time and mitral inflow E velocity to tissue Doppler E' velocity ratio (E/E'), mitral flow propagation velocity (Vp), ratio of mitral inflow to Vp (E/Vp) were measured.
Myocardial color coded tissue Doppler images (TDI) were acquired from apical 2-, 3-, and 4-chamber views. Gain settings, filters, and pulse repetition frequency were adjusted to optimize color saturation. Sector size and depth were optimized for the highest frame rate (> 100 fps). Three consecutive beats were stored, images were analyzed offline with a commercial software (Echopac 6.3.4, Vingmed, General Electric, Horten, Norway). Longitudinal myocardial velocities were acquired from six basal segments. For timing, onset of QRS complex was used as a reference point, from which time to peak early diastolic velocity (Te) and peak systolic velocity (Ts) were calculated for each segment. Diastolic and systolic delays were evaluated with maximal temporal difference between Te and Ts of 6 basal segments (TeDiff and TsDiff, respectively).8) Higher values would indicate more severe dyssynchrony. Echocardiographic examination was also performed for 24 demographically matched control group and results were compared with the patients. Two dimensional echocardiography and TDI measurements were repeated at 6-month follow-up to determine temporal evolution of dyssynchrony and LV volumes after STEMI. LV functional improvement was described as any increase in EF and positive remodeling was described as 15% increase in ESVI compared with baseline values.9)
Echocardiographic examinations were performed by the same observer blinded to patients' clinical statuses. Intra-observer reliability of TeDiff, EDVI, and ESVI measurements was tested in 10 randomly selected examinations. Intraclass correlation coefficients of TeDiff, EDVI, and ESVI were 0.92 [95% confidence intervals (CI) 0.76–0.96], 0.90 (95% CI 0.75–0.93), and 0.91 (95% CI 0.72–0.95), respectively.
Statistical analysis
Continuous variables were presented as means ± standard deviations. Control group was matched with study group using propensity score matching. Adjusted propensities were calculated using logistic regression analyses of demographic characteristics of patients and controls. Comparison between controls and the patients was performed with Student t-test. Comparison between baseline and 6-month echocardiographic findings were performed using paired samples t-test. Categorical variables were presented as numbers and percentages and compared with chi-square or Fishers' exact test. Correlations of DD with other echocardiographic parameters were measured with Pearson test. In order to find independent predictors of systolic functional improvement and remodeling of LV, logistic regression analyses that include baseline patient characteristics such as age, gender, presence of hypertension, presence of diabetes, symptom onset to balloon time, cardiac biomarkers, localization of myocardial infarction and baseline EF, together with characteristics that were significant in univariate analysis were performed. Two sided p value less than 0.05 was considered statistically significant. Statistical data analysis was performed with Statistical Package for the Social Sciences (SPSS for Windows version 11.0, SPSS Inc., Chicago, IL, USA).
Results
Study population
Fifty two consecutive patients were included in the study according to predefined criteria. Two patients who presented with subacute stent thrombosis after hospital discharge and 2 patients who did not attend 6 month follow-up were excluded from the analysis. Clinical and echocardiographic follow-up of 48 patients constituted the study population (Table 1). All patients underwent successful revascularization with thrombolysis in myocardial infarction flow grade III in infarct related artery. Infarct related artery was left anterior descending artery in 23 (48%), right coronary artery in 20 (42%) and circumflex artery in 5 patients (10%). Twenty patients (42%) had multivessel disease which was described as more than 50% diameter stenosis of any or both of non-infarct related arteries. Majority of cases presented without signs of heart failure (Killip class I: 46 patients, class II: 1 patient, class III: 1 patient). Median symptom onset to balloon time was 193 minutes (interquartile range: 135–254). Baseline characteristics of study patients and healthy controls were comparable. Expectedly, study group had significantly lower LV EF and DT, whereas they had significantly higher TsDiff and TeDiff compared to control group.
Correlation of TeDiff with other echocardiographic parameters
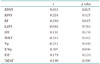
We conducted an analysis to search for any relationship of baseline TeDiff with other baseline echocardiographic parameters. TeDiff was found to be correlated, at moderate level, negatively with EF and positively with E/Vp (Table 2). Other echocardiographic parameters did not show any significant correlation with TeDiff.
Follow-up findings
At 6 months, 42 patients (88%) were asymptomatic (4 patients had class II, 2 patients had class III functional capacity). Complete revascularization was achieved in 39 patients (81%), whereas 4 patients (8%) required target vessel revascularization during follow-up. Medical treatment of the study population was generally in line with recent guidelines (incidence of aspirin, clopidogrel, renin-angiotensin-system inhibitor, beta blocker and statin use at 6 months were 88, 90, 85, 90, and 52%, respectively). Echocardiographic findings at follow-up revealed that study patients showed improved systolic function (from 50.9 ± 7.6 to 55.1 ± 8.1%, p = 0.001), via increasing their EDVI (from 58.7 ± 12.5 to 63.9 ± 16.1 mL/m2, p = 0.001), while ESVI remained unchanged (from 29.0 ± 8.4 to 29.1 ± 10.5 mL/m2, p = 0.892). LAVI did not change significantly either (from 18.6 ± 7.9 to 19.6 ± 6.9 mL/m2, p = 0.249).
Incidence of diastolic dyssynchrony and relationship with remodeling
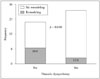
Upper reference limit of TeDiff in control group was calculated from (mean + 1.96 × standard error of mean) formula. It was found to be 29 ms. When ≥ 29 ms was considered as a cutoff value, 58% of patients with STEMI would have DD, as compared to 33% in heathy individuals (p = 0.046). Using the same cutoff value, DD would be prevalent in 52% of cases at 6 months.
Baseline TeDiff was significantly higher in STEMI group than that of controls (Fig. 1). TeDiff did not change significantly during follow-up in study group, whereas difference between 6 month follow-up and controls remained borderline.
Baseline TeDiff was not correlated with change in ESVI, EDVI or LAVI at 6 months. However there was a positive correlation with change in EF at 6 months (Fig. 2). Furthermore, remodeling developed significantly less in patients with baseline DD compared to patients without baseline DD (Fig. 3). Independent predictors of EF improvement were found to be baseline EF [odds ratio (OR) 0.844, 95% CI 0.746–0.955, p = 0.007] and serum CK-MB level (OR 0.99, 95% CI 0.984–0.998, p = 0.008), whereas independent predictors of LV remodeling were found to be DT (OR 0.971, 95% CI 0.945–0.998, p = 0.034), CK-MB (OR 1.011, 95% CI 1.000–1.022, p = 0.059), and TsDiff (OR 1.062, 95% CI 1.018–1.108, p = 0.006) with logistic regression analyses.
Effect of chronic ischemia on diastolic delay
Baseline TeDiff of patients with single vessel and multi vessel disease was not different (36.2 ± 21.7 ms vs. 35.6 ± 17.6 ms, p = 0.922). Incidence of DD was similar between two groups as well (50% vs. 65%, respectively, p = 0.302). Effect of complete revascularization on TeDiff was found to be neutral (37.9 ± 20.8 ms from baseline to 39.8 ± 24.0 ms at 6 months, p = 0.763). TeDiff of patients at follow-up with and without complete revascularization did not differ either (35.7 ± 19.1 ms vs. 36.8 ± 24.3 ms, respectively, p = 0.890).
Discussion
Few data exists concerning DD itself. Today most of our knowledge about DD comes from heart failure studies, although left bundle branch block alone is known to cause DD.7)10)11) The incidence of DD was reported as high as 46% to 69% in systolic heart failure11)12)13) and 36% in diastolic heart failure.14) Although DD is more frequent in patients with wide QRS complex (> 120 ms), considerable proportion of patients with DD have narrow QRS complex. Besides, correlation between DD and QRS duration is weak,12)13) suggesting mechanisms other than electromechanical delay take place.
Systolic dyssynchrony may cause DD, i.e., segments with delayed contraction are expected to show delayed relaxation. Attenuation of diastolic and systolic dyssynchrony in cardiac resynchronization therapy responders suggests this interrelationship.13) However we have found that level of diastolic and systolic dyssynchrony (TsDiff and TeDiff) were not correlated with each other in patients with STEMI. Impaired diastolic function such as low myocardial early diastolic velocity or high E/E' was proposed as a determinant of DD in some studies.8)10) Similar to those studies, we found E/Vp ratio to be positively correlated with TeDiff. Further, LV systolic function was negatively correlated with TeDiff. DD can also develop as a result of myocardial disease of any etiology. Probably the most common form is hypertensive heart disease. DD was more frequent in hypertensive patients compared to healthy individuals and was associated with diastolic dysfunction and LV remodeling.15) Relatively higher incidence of DD in our control group might be associated with high incidence of hypertension as well. Other common etiology is myocardial ischemia which can lead to mechanical dyssynchrony of LV (both systolic and diastolic) especially in patients with preserved EF through a delay in myocyte contraction, relaxation or myocardial scarring.16) Coronary artery disease was was shown to be associated with dyssynchronous regional diastolic function that improved after coronary revascularization in the previous studies.2)17)18) Likewise, our study showed that STEMI causes dyssynchronous diastolic function of LV. Furthermore DD at 6-month follow-up tended to be higher than control group. Incidence of DD was 58% in patients with STEMI, which is significantly higher than in controls (33%). Previously, a study found similar incidence of DD (21%) in patients with hypertension using TDI from 6 basal segments.8) All these suggest that DD is a common finding of diastolic dysfunction and can be encountered in variety of disease settings.
As summarized above, pathogenesis of DD is multifactorial and yet unclear. In addition, which mechanism has the predominance in ischemic heart disease is debatable. In our analysis, we have found TeDiff ≥ 29 ms to be indicative of DD. A previous study described the intraventricular diastolic delay of 36 ms from four basal segments as threshold value.12) More importantly, we have also found that patients with baseline DD (TeDiff ≥ 29 ms) were less likely to develop adverse remodeling at 6 months. Furthermore, baseline TeDiff was positively correlated with change in EF at six months in our analysis. However it must be noted that DD per se was not an independent predictor of either improvement of systolic function or LV remodeling during follow-up. Instead, DD during STEMI stood out as a useful marker of the extent of myocardial injury during acute phase.
As a general rule, the more myocardium is affected the more benefit from timely intervention is possible. So our findings suggest that higher diastolic delay means more myocardial segments affected during STEMI. However, we think DD is not related to true infarct size, which should be associated with late remodeling. Instead, we think DD reflects the area at risk or infarct size plus reversibly injured peri-infarct myocardium that is salvaged with primary intervention, which explains recovery of LV function and infrequency of remodeling thereafter. This is also supported by the finding that diastolic delay was negatively correlated with EF in acute phase. In that sense DD can be a byproduct of LV damage during AMI. In agreement with this we did not find any significant effect of chronic ischemic lesions and revascularization of them on diastolic delay and the incidence of DD, contrary to a previous study.17) Therefore we suggest that it is the peri-infarct stunned myocardium not the presence of ischemia per se that plays major role in the development of DD during STEMI while the extent of infarction is also important. On the other hand, as shown in this study as well as numerous previous ones, systolic dyssynchrony was determined by infarct size and associated with adverse remodeling after AMI.5)6)19)20)21) This may be due to the fact that diastolic function gets impaired earlier than systolic function in ischemia cascade, hence the more myocardial segments are affected by coronary occlusion the more severe or prolonged diastolic delay can be. In addition, myocardial stunning was classically described to improve over days to week, so by the time of echocardiography in first 48 hours some recovery of regional systolic function might have taken place which more or less limits systolic dyssynchrony close to infarct size. However regional diastolic dysfunction might have persisted due to nature of ischemia cascade hence more precisely representing affected myocardial segments. Ultimately, these assumptions and findings need to be supported by future studies investigating different mechanisms of DD to predict LV recovery in patients with AMI.
Study limitations
There were some limitations inherent to TDI technique. TDI method is angle dependent and can only assess longitudinal motion. Apart from longitudinal motion, TDI is unable to differentiate active contraction from passive tethering of adjacent segments. Strain and strain rate analysis would be more precise to identify true wall contractions.
This study was underpowered to detect significant changes in TeDiff during follow-up period during which it tended to decrease. In addition, a larger study population could allow us to propose a cutoff value of TeDiff for the prediction of adverse remodeling.
Finally, data on the effect of chronic ischemia and later revascularization on DD should be viewed with caution as this study was not designed to investigate this issue. Limitations are 1) timing of revascularization procedure was variable among the patients (different approaches are possible: in hospital or elective or symptom driven revascularization), 2) some patients needed unplanned target vessel revascularization, 3) some of them could not be completely revascularized at all, and 4) medical treatment was not standardized across the study population.
Conclusion
There are two main results of this study. 1) Even properly treated STEMI disrupts the diastolic synchronicity of LV, and DD was observed frequently (58%) in patients with STEMI. 2) DD induced by STEMI is associated with less remodeling during follow-up and baseline TeDiff was positively correlated with improvement in global LV systolic function. These findings suggest that DD is associated with peri-infarct stunned myocardium that is salvaged with primary intervention as well as infarct size.



 XML Download
XML Download