

 PDF
PDF ePub
ePub Citation
Citation Print
Print


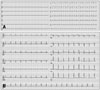
I read with interest the paper by Yoo et al.,1) published in the March, 2016 issue of the Journal, about the 41-year-old previously healthy woman, who suffered Takotsubo syndrome (TTS) complicated by cardiogenic shock, necessitating resuscitation and invasive supportive means of extra-corporeal membrane oxygenation, with eventual full recovery of her heart function. The patient's first electrocardiogram (ECG) (Fig. 1A) recorded on her 2nd visit to the hospital, showed low QRS complexes, in keeping with a recent report,2)3) associating transient attenuation of the ECG QRS complexes (attQRS) and TTS. It is difficult to compare this ECG with the one recorded 1month after discharge (Fig. 1B), since the upper panel of the figure has half of the height of the lower panel, but it appears that there was decrease in QRS voltage in all ECG leads of the admission ECG. This transient attQRS has been attributed to myocardial edema (ME),2) as diagnosed by cardiac magnetic resonance imaging (cMRI).4)5) Unfortunately there was no cMRI in this case, early during the clinical course corresponding to the ECG in Fig. 1A, but much later, a month after admission,1) which of course showed no ME. I will be grateful to the authors if they provide us with information about subsequent ECGs during the patient's follow-up, or ECGs recorded before her admission with TTS (unlikely in a previous healthy young woman), regarding the amplitude of the QRS complexes in those ECGs, in comparison with the ECG of Fig. 1A.
See the article "".
See the reply "Response to Letter Regarding Article, "Stress-Induced Cardiomyopathy Presenting as Shock"" in Volume 24 on page 180.
Figures and Tables
References
1. Yoo TK, Lee JY, Sung KC, Oh SS, Song YS, Lee SJ, Ko KJ. Stress-induced cardiomyopathy presenting as shock. J Cardiovasc Ultrasound. 2016; 24:79–83.
2. Madias JE. Transient attenuation of the amplitude of the QRS complexes in the diagnosis of Takotsubo syndrome. Eur Heart J Acute Cardiovasc Care. 2014; 3:28–36.
3. Guerra F, Giannini I, Pongetti G, Fabbrizioli A, Rrapaj E, Aschieri D, Pelizzoni V, Villani GQ, Madias JE, Capucci A. Transient QRS amplitude attenuation is associated with clinical recovery in patients with Takotsubo cardiomyopathy. Int J Cardiol. 2015; 187:198–205.
4. Migliore F, Zorzi A, Marra MP, Basso C, Corbetti F, De Lazzari M, Tarantini G, Buja P, Lacognata C, Thiene G, Corrado D, Iliceto S. Myocardial edema underlies dynamic T-wave inversion (Wellens' ECG pattern) in patients with reversible left ventricular dysfunction. Heart Rhythm. 2011; 8:1629–1634.
5. Perazzolo Marra M, Zorzi A, Corbetti F, De Lazzari M, Migliore F, Tona F, Tarantini G, Iliceto S, Corrado D. Apicobasal gradient of left ventricular myocardial edema underlies transient T-wave inversion and QT interval prolongation (Wellens' ECG pattern) in Tako-Tsubo cardiomyopathy. Heart Rhythm. 2013; 10:70–77.
 XML Download
XML Download