

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Pericardial cysts are rare, usually benign congenital anomalies but may also be acquired. They represent 6% of mediastinal masses and 33% of all mediastinal cysts.1) The vast majority are asymptomatic and are usually found incidentally on chest radiographs, computed tomography scans, magnetic resonance images, or echocardiography.2) Large pericardial cysts may cause compression on adjacent structures and organs, resulting in dyspnea, chest pain, or persistent cough.3) There have been reports of cyst rupture, cardiac compression, atrial fibrillation, and even sudden cardiac death from these cysts, although these complications are uncommon.4) A 55-year-old Italian dialysis patient with a shortness of breath, asthenia and excessive fatigability was referred to our institution. He had history of pericarditis, myocarditis and massive pleural effusion. His electrocardiogram showed sinus rhytm. Transthoracic echocardiography (TTE) revealed normal left and right ventricular systolic performance, with normal wall thicknesses and chamber sizes and a pericardial thickening. Color Doppler imaging showed a mild mitral and tricuspid regurgitation. Apical and subcostal views of TTE showed an oval echolucent structure at the right cardiophrenic angle, minimally compressing the right atrium, and of approximately 10 × 4 cm, consistent with a pericardial cyst (Fig. 1). Cardiac magnetic resonance (CMR) confirmed echocardiography findings, showing the presence of the pericardial cyst with several fibrinous strands inside associated with right-sided massive pleural effusion. Late gadolinium-enhanced CMR images showed intramural myocardial enhancement in anterior and inferior wall and enhancement of pericardium, as an expression of myocardial and pericardial inflammation (Fig. 2). The patient was treated conservatively because of high surgical risk attributed to severe kidney failure. A repeated TTE with the apical 4-chamber view at 20 months later showed minimal increase in the size of the pericardial cyst. The discovery of a pericardial cyst obliges the clinician to perform a broad differential diagnosis with a coronary artery aneurysm, dextrocardia, malignancy, and even pneumonia.5) CMR may help in this diagnosis.
Figures and Tables
Fig. 1
Echocardiographic evaluation revealed a pericardial cyst in the inferior wall of the left ventricle.
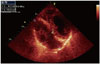
Fig. 2
Vertical long-axis (A and D) and short-axis (B, C, E, and F) cardiac magnetic resonance (CMR) images of pericardial cyst in patient with pericarditis, myocarditis and massive pleural effusion. Cyst (white asterisks) has low signal intensity on T1-weighted spin-echo CMR image (F) and high signal intensity on T2-weighted short tau inversion-recovery spin-echo CMR image (C). Steady-state-free procession cine CMR images (A and B) show several fibrinous strands in the cyst and right-sided massive pleural effusion (black asterisks). Late gadolinium enhanced CMR images (D and E) show intramural myocardial enhancement in anterior and inferior wall (white arrows) and enhancement of pericardium (white arrowheads), as an expression of myocardial and pericardial inflammation.

References
1. Patel J, Park C, Michaels J, Rosen S, Kort S. Pericardial cyst: case reports and a literature review. Echocardiography. 2004; 21:269–272.
2. Patel S, Hajmedi P, Fischbein J. Common symptoms with rare entity: a giant pericardial cyst. Am J Med. 2015; 128:e27–e28.
3. Seo GW, Seol SH, Jeong HJ, Seo MG, Song PS, Kim DK, Kim KH, Kim DI, Kang MJ, Kim JY. A large pericardial cyst compressing the left atrium presenting as a pericardiopleural efussion. Heart Lung Circ. 2014; 23:e273–e275.
4. Aksu U, Kalkan K. Pericardial cyst hydatid rupture complicated by pericardial tamponade. Int J Cardiol. 2015; 193:62–63.
5. Hamad HM, Galrinho A, Abreu J, Valente B, Bakero L, Ferreira RC. Giant pericardial cyst mimicking dextrocardia on chest X-ray. Rev Port Cardiol. 2013; 32:49–52.
 XML Download
XML Download