

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Echocardiographic assessment of left ventricular (LV) contractility and dimensions is important in the management of patients with congenital heart disease. Conventional two-dimensional (2D) measures are limited because of volume or pressure-overloaded right ventricles that may distort the septal planes.1) Both M-mode and 2D echocardiography make important geometric assumptions about the LV which leads to inaccuracies in measurements. There is also poor inter- and intra-observer variability which limits the use of the technique in follow up of patients and also in scientific studies.2) Introduction of real time three dimensional echocardiographic (RT3DE) imaging techniques is of great interest since this methodology may circumvent many of the above mentioned limitations.3) Validation of the analysis of LV ejection fraction (EF) and volumes using RT3DE has been demonstrated in previous studies that used magnetic resonance imaging.4)5)6)7) Cardiac magnetic resonance (CMR) is not universally available, is not practical in many situations, is expensive, and is a relative contraindication in patients with pacemakers.8) Historically, the determination of the LV volume is obtained by cardiac angiography.9) CMR is very expensive for our patients and not so widely available in our country. So, we aimed to study the validity of RT3DE as a non-invasive cardiac imaging method for measurement of LV volumes using cardiac angiography as the reference technique in group of patients with tetralogy of Fallot (TOF) referred for cardiac catheterization in our institute.
Methods
Study population
The study included 40 children with TOF who were referred to undergo cardiac catheterization with angiography as part of their pre-surgical assessment. In our institute, patients with TOF are referred for cardiac catheterization as part of their preoperative assessment if there is question about stenosis of the peripheral pulmonary artery, presence, origin, and insertion of major aortopulmonary collateral arteries which should be documented. Those with previous systemic-to-pulmonary artery shunting need cardiac catheterization for visualization of the shunt and the pulmonary artery at the shunt insertion site. Sometimes assessment of coronary artery anatomy is needed.
Patients with associated pulmonary atresia or aortic arch abnormalities were excluded. Eighteen healthy, age and sex matched children were included in this study as a control group. The controls were subjected to 2D and three dimensional (3D) echocardiography to estimate LV volume aiming to compare with that of the studied cases. Informed consent was obtained from the children's guardians. The study was approved by the Institutional Research Committee.
Methods
All patients were subjected to thorough history taking and detailed clinical examination, 2D echocardiography, and cardiac catheterization.
2D echocardiography
Echocardiography was performed for all cases and controls in a supine, left lateral position using a Vivid-7 machine (GE Medical, Horten, Norway) system with probe 3 or 5 MHz (multifrequency transducer) according to the age of patient. M-mode measurements were done at the level of the tips of the mitral valve leaflets in the parasternal long-axis view of the LV. The parameters measured in systole and in diastole included: LV dimensions (LV end diastolic dimension, LV end systolic dimension, LV posterior wall thickness), right ventricular diameter, and interventricular septum fractional shortening and EF were also calculated.
RT3DE
It was performed by GE-Vivid 7 ultrasound system using the technology of the 3000 element matrix probe (3V probe). This electronic sector probe consisting of X4-2 or X7-2 matrix phased array transducer (center frequency of 2–4 MHz). Ultrasound images of the ventricle were calculated using Tom Tec 4D Cardio-View RT 1.2 software (GE Medical, Horten, Norway).
RT3DE imaging was performed from the apical window with the patient either in supine or in the left lateral decubitus position. Full LV volume acquisitions were performed over 4 cardiac cycles. Tomtec plug-in was initiated after 3D acquisition. RT3DE data files were analyzed with semi-automatically determined optimal geometry (multiplanar reconstruction to define LV long axis).
After adjustment of the long axis of the ventricle, the initial contour is made on the end systolic and end-diastolic frames of the extracted 4-chamber view from a small set of 6 initial points. LV endocardial contours were traced in every slice semi-automatically frame by frame, with the papillary muscles and trabeculae included in the LV cavity. These contours were corrected manually when necessary and then used to reconstruct for each phase of the cardiac cycle the endocardial surface in the 3D space. These reconstructed surfaces were used to calculate LV volume over time throughout the cardiac cycle. Each volume curve was analyzed to obtain end-diastolic (EDV) and end-systolic (ESV) volumes that were identified as the maximum and minimum values, and EF was computed. The algorithm calculated and displayed automatic contours for the 2-chamber in the long-axis views. When the detected boundary is approved, the tool provides both global and segmental information including EDV, ESV, systolic volume, and EF (Fig. 1). The mean analyzing time was calculated.
To determine the reproducibility of LV volume measurements for RT3DE, image analysis was repeated in a random sample of 15 patients by an additional investigator as well as by the same primary reader at least 1 week later. During these repeated analyses, the investigators were blinded to the results of all prior measurements. Inter- and intra-observer variability was calculated as the absolute difference of the corresponding pair of repeated measurements in percent of their mean in each patient and then averaged over the 15 patients.
Biplane cineangiography
It was obtained in long axial projections (right anterior oblique 30° in frontal position and left anterior oblique 60° with 20° cranial angulation in lateral position) at 35 frames/sec. LV volume was calculated using the following equation assuming that LV geometry approximated with considerable accuracy by an ellipsoid. Correction for image magnification and distortion from non-parallel X-rays was performed according to the method of Greene et al.10)
LV end diastolic volume (LVEDV) = 4/3 π [(L/2) (M/2) (N/2)] = π/6 (LMN)
Where V is the LV volume, L is the long axis, M is the short axis in one plane and N is the short axis in the other plane.10)
Then, LVEDV index (LVEDVI) was calculated by dividing LVEDV by body surface area.11)
Results
The study included 19 males (47.5%) and 21 females (52.5%). Fourteen patients were offspring of consanguineous marriage. Their mean age was 3.0 ± 1.8 years; their age ranges between 11 months and 8 years with median 2.35 years, their mean weight was 12.9 ± 3.4 kg, and their mean body surface area was 0.5 ± 0.1 m2. The control group included 18 children with age ranged between 10 months to 6.5 years, median age 2.5 years. The group included 10 females (56%) and 8 males (44%).
Table 1 shows the demographic, echocardiographic data including conventional echocardiography and RT3DE and the angiographic data of the included patients. Two cases (5%) only had LVEDVI between 20–30 mL3/m2 and the remaining 38 cases (95%) had a volume > 30 mL3/m2.
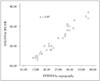
There was a good correlation between RT3DE and cineangiography for estimation of LVEDVI in all studied patients (r = 0.97, p < 0.001) (Fig. 2). Bland-Altman plot shows the comparison between the LVEDVI by RT3DE and angiography (Fig. 3). Bias was -2.6, SD was ± 1.96. The upper limit of agreement was 3.1 and the lower limit of agreement was -8.3.
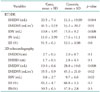
We compared the 2D and RT3DE echocardiographic findings of both cases and controls as shown in Table 2. LVEDV measured by RT3DE in the studied TOF cases was with a mean value of 22.5 ± 7.4 mL3. The mean LVEDV of the studied TOF cases was less than that of control group, whose mean value was 33.3 ± 19.99 mL3. These results showed clearly that LV volume was less than normal in most of our patients. Statistical analysis showed that there was a significant difference between LVEDV measured by RT3DE in the studied TOF patients and that of control group (p < 0.004) as shown in Table 2.
There was significant under estimation of LVEF by RT3DE echocardiography in comparison to 2D echocardiography (p < 0.001).
Measurement was done without any manual corrections in 5 patients (13%), and with manual corrections in 35 patients (87.5%). The mean analyzing time was 20 min per case.
Intraobserver variability with RT3DE was low (1.9%) while the interobserver variability was acceptable as well (3.7%).
Discussion
We aimed to correlate the RT3DE as a non-invasive tool of assessment of the LV with the biplane angiography as a reference standard tool.
In our study, the LVEDV and the LVEDVI of our TOF patients were significantly lower than controls. The LV in infants and children with TOF is often smaller than normal but rarely hypoplastic.12) The development of the LV muscle fibers was correlated with the volume of pulmonary blood flow or LV inflow volume in children with TOF.13)
The LV volume determined with RT3DE was strongly correlated with that assessed by angiography which was as reported by other investigators.9) LVEDV estimated by RT3DE was smaller than that estimated by angiography. This mild underestimation was explained by various reasons. First, the patient's respiratory movement was difficult to control to acquire RT3DE images. Secondly, the transducer was positioned in only an apical acoustic window. Technically, to acquire a RT3DE data set, the whole LV cavity could not always be placed within the image angle.9) Also this is near to the study done by Heusch et al.14) who denoted that LVEDV measured by RT3DE was smaller than those calculated from the angiocardiography but the correlation between the two methods is good (r = 0.93, p = 0.0001).
The above data clearly illustrates that RT3DE can be used as a reliable method for accurate estimation of left heart volume in children.
2D echocardiography alone cannot be used for assessment of the LV volume because 2D echocardiography measures single ventricular dimension rather than a ventricular volume. This dimension can give a good impression of cavity size but less accurate for precise quantification of LV volume.15)
In our study, LVEF measured by RT3DE was significantly underestimated in comparison to that measured by 2D echocardiography, which suggested that RT3DE underestimate EF when compared to 2D echocardiography. This was also reported by other investigators. The reason for this underestimation may be that RT3DE cannot consistently differentiate between the myocardium and the trabeculae. So, it is recommended to trace the endocardium to exclude trabeculae in the LV cavity for 3D echocardiography. As well, one-beat acquisitions may not successfully capture true end-systole, because of the reduced temporal resolution. This will lead to inaccurate ESV calculations and EF measurements.16)
The study was limited by being performed for patients with only TOF and not other types of congenital heart disease. So, we need future studies in other types of congenital heart disease. In addition, the only available RT3DE transducer had an operating frequency of 2–4 MHz. Finally, the software require manual tracing of the endocardial boundaries so, introduction of automated border detection, if accurate, would make this technique easier, faster and more feasible in the future.
In conclusion, in patients with good acoustic windows, RT3DE using state-of-the-art technology provides accurate and reproducible measurements of global LV volumes.



 XML Download
XML Download