

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atrial fibrillation (AF) is the leading cause of stroke.1) However, a few studies suggest that some of AF may be a result from stroke. Previous studies reported paroxysmal or asymptomatic AF after acute ischemic stroke had already occurred, in patients without previous history of AF. Incidental impairment of autonomic nervous system, which is reported in upto 40% of acute ischemic stroke patients, may trigger a new onset AF.2)3)4)5) Also, various cardiovascular diseases accompanied with stroke could attribute to arrhythmogenic remodeling of left atrium (LA), promoting AF.6)7)
AF in acute ischemic stroke patients is associated with higher in hospital mortality and poorer neurological outcomes. More severe neurologic deficits with higher recurrence rates have been reported in stroke patients with AF.8) Therefore, identification of post stroke AF in patents without previous history of AF is important as appropriate anticoagulation could reduce recurrences rates of stroke. However, due to often paroxysmal and asymptomatic nature of AF, patients with post stroke are often underdiagnosed. Also, no consensus has been made for efficient strategies to detect post stroke AF. The 24-hr electrocardiograph (ECG) recording is most often used to screen for AF, however, the sensitivity is relatively poor, detecting previously undocumented AF in only about 2–10.7% of acute ischemic stroke patents.9)10)11)12) Although longer periods of monitoring increases detection rates of post stroke AF, not all patients can undergo extended rhythm monitoring in real world. Therefore, establishing adequate risk stratification tool to select high risk group to undergo extended monitoring could be cost effectively improve detection rate of post stroke AF.
The global LA longitudinal strain (LALS) assessed by two-dimensional (2D) speckle tracking transthoracic echocardiography (TTE) is a relatively simple and reproducible technique, which measures deformation of LA to assess LA function.13) Recent studies have shown that global LALS is well associated with AF recurrences after ablation or cardioversion of AF.14)15)16)17)
In this study, we aimed to investigate if clinical and echocardiographic parameters were associated with post stroke AF in acute ischemic stroke patients without previous history of AF, by comprehensive evaluation of stroke severity and LA structure and function using 2D speckle tracking imaging.
Methods
Study subjects
We analyzed a retrospective cohort of 279 patients with acute ischemic stroke who were referred to the cardiology division for transesophageal echocardiography (TEE) from April 2012 to June 2013. All patients underwent TTE and TEE, as a part of a standard evaluation for the detection of cardioembolic sources within one week of the initial stroke. Ischemic stroke was confirmed by a focal neurologic deficit of sudden onset and magnetic resonance imaging findings. Patients with a transient ischemic attack and negative imaging findings were excluded. Patients who had significant valvular dysfunction to a moderate or severe degree, previous history of valve repair, valve replacement, cardiomyopathy, AF, supraventricular tachycardia, or radiofrequency ablation on the LA were not included in this study. Finally, the stored images were analyzed in 227 acute ischemic stroke patients without previous history of AF who presented with sinus rhythm at time of admission.
Patient clinical data, including history of hypertension, diabetes mellitus, cigarette smoking, dyslipidemia, a previous cerebrovascular accident, AF, onset of stroke, and neurologic examination including National Institute of Health Stroke Scale (NIHSS) score were determined at the time of admission. The diagnosis of previous persistent and paroxysmal AF was made on the basis of patient recall or by documentation of the arrhythmia on a previous ECG or medical record when available. The subtypes of ischemic stroke were classified according to the Trial of Org 10172 in Acute Stroke Treatment criteria by neurologists.18)
Every patient underwent immediate and continuous ECG monitoring for at least 3 days after admission. After discharges, patients underwent 24-hr ECG from outpatient clinics if patients complained symptoms of palpitation. Post stroke AF was defined as newly diagnosed AF after acute ischemic stroke in a patient.
Risk of post stroke AF was assessed using the CHA2DS2-VASc score, which assigns one point for congestive heart failure within the past 3 months or left ventricular (LV) ejection fraction < 40%; one point for hypertension; two points for age > 75 years; one point for diabetes; two points for stroke, transient ischemic attack, or systemic embolism; one point for vascular disease (prior myocardial infarction and peripheral arterial disease); one point for age 65 to 74 years; and one point for female sex.19) The two points derived from the acute embolism vent causing the present admission were not added to the patient.
Conventional transthoracic echocardiography
Each patient underwent a comprehensive transthoracic echocardiographic study using a Vivid 7 or Vivid 9 cardiovascular ultrasound system (GE Medical Systems, Horten, Norway), equipped with 2.5–3.5 MHz phased-array sector probes. During echocardiography, a one-lead ECG was recorded continuously. Standard 2D and Doppler measurements were performed per the recommendations of the American Society of Echocardiography guidelines. For the assessment of LA volume, apical four-chamber and two-chamber views were obtained. Maximal LA volume was measured manually using Simpson's methods at the end of ventricular systole and indexed to the body surface area.20)
Pulsed Doppler echocardiography of the transmitral flow was performed. The sample volume was positioned at the level of the mitral tips in the apical four-chamber view. Images were recorded at a speed of 50 to 100 mm/sec. From the transmitral recording, the peak early (E) and late diastolic filling velocities were obtained. An apical four-chamber view was also used to obtain Doppler tissue imaging of the mitral annulus. Sample volumes were placed on the septal side of the mitral annulus. Values shown for systolic, peak early (e'), and late diastolic annular velocities were obtained.
Speckle tracking echocardiography
Each patient underwent a 2D speckle echocardiography of the LA. Three consecutive cardiac cycles were recorded and averaged, and the frame rates were set to 60 to 80 frames/sec. The cardiac cycle was demarcated by indicating QRS onset and QRS complex used as the first reference frame. The analysis was performed offline using customized software (EchoPAC PC; GE Medical Systems). The LA echocardial border was manually traced in both four-chamber and two-chamber views. Because two segments of the LA roof demonstrated a lower longitudinal strain curves than those of the other four, they were excluded from both the four-chamber and the two-chamber views.21)22) Therefore, global peak LALS during the ventricular systole was then measured by averaging the values obtained in the eight other LA segments. The time to peak LALS is also measured as the average of the eight segments and by calculating the time delay from the QRS to the positive peak LALS.
An experienced cardiologist, who was unaware of the patients' information, analyzed all echocardiographic values. The intra-observer and inter-observer reproducibility for the assessment of global LALS were determined by the Bland-Altman analysis. Intra-observer reproducibility was determined by repeating the strain measurements at two different time points by one experienced reader in 15 randomly selected patients. A second experienced reader performed the strain analysis in the same 15 patients, providing the inter-observer data. The Bland Altman analysis and intra-class correlation coefficient (ICC) showed good intra-and inter-observer agreement for global LALS. For inter-observer agreement of global LALS, the mean difference was 1.7 (-1.3, 4.4) and the ICC was 0.88; for intra-observer agreement, the mean difference was 1.2 (-2.0, 3.1) and the ICC was 0.90.
Transesophageal echocardiography
Each patient underwent comprehensive TEE immediately after the TTE by using a 5- to 7-MHz multiplane probe positioned at the appropriate level within the esophagus. All examinations were recorded on digital video in real time for display and evaluation. The TEE images were independently reviewed by two experienced cardiologists.
The multiple standard tomographic planes were imaged and LA appendage (LAA) emptying velocity, the presence of LA or LAA thrombi, presence of patent foramen ovale, and the severity of spontaneous echo contrast (SEC) in the LA or LAA were determined. Peak LAA emptying velocities were measured using pulsed Doppler by placing the sample volume approximately 1 cm inside of the orifice of the LAA.23) The peak emptying wavelets were measured in three consecutive cycles, and the maximal velocities were then averaged. An LA or LAA thrombus was diagnosed by the presence of an echo-dense mass in the LA or LAA, distinct from the endocardium and the pectinate muscles of the LAA.24) The SEC was diagnosed by the presence of characteristic dynamic smoke-like swirling echo in the LA or LAA, distinct from the background white noise due to excessive gain.25) The severity of the SEC was classified into one of the four grades on the basis of appearance and density as follows: none, mild (minimal echogenicity detectable only with optimal gain settings transiently during the cardiac cycle), moderate (a dense swirling pattern during the entire cardiac cycle), or severe (intense echogenicity and very slow swirling patterns in the LA or LAA, usually with a similar density in the main cavity).26)
Statistical analysis
Continuous variables were presented as a mean ± standard deviation and categorical variables as absolute and relative frequencies (%) of the group total. Comparisons between groups were performed using χ2, Kruskal-Wallis, or Mann-Whitney U tests. We constructed the receiver operating characteristic (ROC) curves to determine the diagnostic ability of global LALS and CHA2DS2-VASc score for post stroke AF. The performance of the predictive selected parameters was assessed using the area under the ROC curve and diagnostic performances were compared by means of the Delong tests.27) Associations between clinical/echocardiographic parameters and post stroke AF were assessed using univariate and multivariate logistic regression analyses. Variables selected for entry into the analysis were those with p < 0.1 on the univariate analysis and important variables in previous studies. The incremental predictive value of the global LALS for post stroke AF was assessed in three modeling steps. The first step consisted of CHA2DS2-VASc, a composite risk from the clinical variables. Then, NIHSS and LA volume index were added sequentially. The model χ2 value was used to determine whether there was a difference between various nested models for predicting the end point. The incremental value was assessed by comparing the global χ2 value for each parameter. The prognostic value of global LALS was determined using the Cox proportional-hazards model. A two-sided p value < 0.05 was accepted as indicating statistical significance. All data were analyzed using IBM SPSS Statistics for Windows version 21.0 (IBM Corp, Armonk, NY, USA).
Results
Clinical characteristics
Post stroke AF occurred in 25 patients (11%) during mean follow up of 23 ± 8 month. Table 1 shows baseline clinical characteristics of patients with or without post stroke AF. Patients with post stroke AF were significantly older than those without post stroke AF (p < 0.01). There was no statistically significant difference in the distribution of gender or comorbidities. The median value of CHA2DS2-VASc score did not differ between two groups. The NIHSS score was significantly higher in patients with post stroke AF.
Echocardiographic characteristics
Echocardiographic parameters are described in Table 2. The LA volume index and global LALS were significantly different between two groups. Patients with post stroke AF were presented with significantly higher LA volume index and lower global LALS. The LV ejection fraction and LV diastolic function, reflected by E/e', did not show significant difference.
Clinical and echocardiographic factors in association with post stroke AF
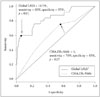
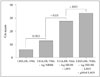
The global LALS < 14.5% identified post stroke AF with are under curve of 0.837 (sensitivity = 60%, specificity = 95%). The ROC analysis showed comparable value for LA volume index > 32 mL/m2 with area under cover of 0.752 (sensitivity = 76%, specificity = 69%) with no significant difference for diagnostic performance (p = 0.42). Global LALS showed significantly better predictive value for post stroke AF (p = 0.02) than that of CHA2DS2-VASc (area under the curve = 0.612, sensitivity = 76%, specificity = 45%, p = 0.07) (Fig. 1). The global LALS, LA volume index, log NIHSS and CHA2DS2-VASc ≥ 4 were significantly related to occurrence of post of AF. The global LALS provided incremental predictive values for post stroke AF over combination of clinical variables (CHA2DS2-VASc, log NIHSS) and LA volume index (Fig. 2). From multivariate analysis, only the global LALS was significantly associated with post stroke AF (hazard ratio 0.90, 95% confidence interval 0.83–0.97, p < 0.01) (Table 3).
Discussion
To our knowledge, this is the first study to investigate global LALS for prediction of post stroke AF in patients with acute ischemic stroke. The principal findings in the present study are that impaired mechanical function of LA assessed by 2D TTE with speckle tracking imaging could provide incremental value for predicting post stroke AF in patients with acute ischemic stroke. Therefore, an earlier awareness for high risk patients may improve further detections of post stroke AF, which can lead to appropriate anticoagulation to reduce recurrent stroke.
CHA2DS2-VASc score and global LALS for predicting post stroke AF
Patients with acute ischemic stroke are associated with substantially increased risk of AF. According to previous meta-analysis, 24% of patients with stroke or transient ischemic attack could be diagnosed with post stroke AF.12) Detection of post AF is vital because anticoagulation dramatically reduce risk of stroke recurrence by two-thirds.28) The decision rates of post stroke AF increase with longer and more sequential monitoring of rhythm along with more sophisticated methods, such as implanted loop recorders. However, considering costs and compliance of patients, not all patients with acute ischemic patients could undergo extensive screen of post stroke AF. Therefore, identification of high risk patents for post stroke AF during the course after acute ischemic stroke is important to prevent recurrent stroke. But there are few strategies to establish absolute risk of post stroke AF in patients with acute ischemic stroke with no previous history of AF.
CHA2DS2-VASc score is well validated risk model to estimate the risk of systemic thromboembolism or stroke in patents with AF, which composed of only clinical variables without echocardiographic parameters. Risk factors assigned in CHA2DS2-VASc score are also associated with prevalence of AF.29) Recent studies consistently demonstrated association of AF with advanced age, gender, hypertension, heart failure, diabetes, and myocardial infarctions.30)31)32) In a line with many studies, previous studies suggested that patients with high CHA2DS2-VASc score were associated with increased risk of post stroke AF, even in population without known history of AF.29) Therefore, in our study we used CHA2DS2-VASc score to estimate clinical risks for prevalence of post stroke AF. Interestingly, our results demonstrated better predictive performance of global LALS than that of CHA2DS2-VASc score. Previous study by Schnabel et al.33) suggested that echocardiographic parameters did not improve the risk function for predicting AF in Framingham population, however, their studies relied on M-mode echocardiographic parameters. 2D speckle tracking is an advanced new technique which allows a more direct measurement of LA contractility of endocardium and passive deformation, which well reflects function of LA.13) Structural remodeling of LA from fibrosis is important in pathogenesis of AF, and previous studies showed that the LALS well correlated with fibrosis of LA.16) Usefulness of the LALS is evidenced by several previous studies demonstrating that LA strain well predicts not only AF recurrence after radiofrequency ablation, but also reverse remodeling of LA.4)34)35)36) Overall, our results suggest that global LALS provide additive predictive value to clinical risk predicting tool, CHA2DS2-VASc score for predicting post stroke AF in acute ischemic stroke patients.
Potential clinical applications
The mean value of global LALS of our cohort was 25 ± 8, which is lower when compared to earlier studies demonstrating feasibility of LALS in normal healthy population.37)38) However, considering that age and associated cardiovascular diseases of our cohort, the mean value of global LALS should be lower as atrial function deteriorates with aging and underlying cardiovascular disease. When compared to previous studies regarding LALS in elderly population or in patients with acute stroke or systemic embolism, our result provided similar ranges of global LALS.21)39)
As results from our study demonstrate that global LALS was significant predictor for post stroke AF, patients with lower LALS may benefit from active monitor AF after acute ischemic stroke. Global LALS could provide additive information to select patients who are most likely to benefit from prolonged monitoring of rhythm with implantable loop recorders. Furthermore, the global LALS may provide evidence for initiation of anticoagulation in absence of documented AF in acute ischemic stroke patients. Impairment of LA function reflected by decreased global LALS may attribute to flow stasis in LA, susceptible for thrombus formation. Although further studies are warranted for causal relationships between LA function and post stroke AF, it is possible that functional impairment from various cardiovascular conditions could trigger post stroke AF, which results in further deteriorated function of LA and subsequent thrombus formation. Our results provide evidence for further studies to investigate implication of global LALS for post stroke AF in acute ischemic patients without previous AF.
Study limitations
A few limitations should be addressed in this study. First, this study is a retrospective observational study from a single center, with a limited number of patients who underwent TEE. Second, we have possibly underestimated the true incidence of AF in this population as not every patient underwent rhythm monitoring after discharge. However, all patients who admitted to the stroke unit were under continuous ECG monitoring during hospitalization. Also after discharge, 163 patients underwent serial (more than 1 ECG) ECG and 50 patients had 24 hr Holter from outpatient clinics. Third, as we exclude patients with severe valve diseases to demonstrate association between mechanical function of LA and post stroke AF. This is reflected by relatively low CHA2DS2-VASc of patients in our study. Although this cohort may not represent general population of stroke patients, our data suggest possible application of the global LALS in real world practice.
Conclusion
The global LALS assessed by 2D speckle tracking imaging provides incremental information for predicting post stroke AF over clinical variables, stroke severity, and LA volume index. The global LALS may reflect structural and functional susceptibility for AF, and provide new strategies to better risk stratification for post stroke AF in patients with acute ischemic stroke.



 XML Download
XML Download