

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Transesophageal echocardiography (TEE) is considered to be safe and relatively noninvasive diagnostic tool,1) however severe complications have been reported. The incidence of major TEE-related complications range from 0.2% to 0.5% and mortality is reported to be < 0.01%.2345) Among these complications, problems related to insertion of TEE probe take a large proportion, including perforation of hypopharynx and esophagus.
For our knowledge, there have been reported only few cases of hypopharyngeal perforation, especially not been reported in Asian population to date. We describe the clinical presentations and secondary complications associated with oropharyngeal injury with the case of a 74-year-old man who suffered a hypopharyngeal laceration after TEE.
Case
A 74-year-old man was referred to our cardiovascular center for the evaluation and treatment of mitral regurgitation (MR). He had been complaining of aggravation of dyspnea (New York Heart Association functional class IV) for the preceding 3 weeks, and atrial fibrillation and severe MR were detected from other clinic. The patient had medical history of hypertension and chronic obstructive pulmonary disease for 15 years, and received endovascular aneurysm repair for abdominal aortic aneurysm 8 years ago. He had coronary artery disease and chronic kidney disease, also.
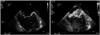
The patient was admitted to the intensive care unit because of uncompensated heart failure and careful control of pulmonary edema with chronic kidney disease. We performed transthoracic echocardiography with subsequent TEE to comprehensive evaluation of mitral valve disease. The patient presented tachypnea and orthopnea before the TEE procedure, less than minimal dose of sedative agent was administrated to lessen patient's discomfort, 1 mg of lorazepam, 25 mg of fentanyl, intravenously. As we checked for the mental status, the patient was not sedate, before and during the insertion of TEE probe. The insertion of TEE probe was performed with the patient in left lateral decubitus position according to the following standardized technique: the probe was inserted through the midline and gently advanced to pass the first pharyngeal curvature corresponding to the base of the tongue. The probe was then extended, and the patient was asked to swallow, at which point the probe was further advanced to enter the esophageal inlet. When the probe has reached to the root of tongue, the patient suddenly changed his position form left decubitus to supine position and gave force to the neck, and resisted to probe insertion. The probe got lodged at right-side of hypopharyngeal area so that failed to advance. At second attempt, TEE probe was advanced into esophagus easily during swallowing with patient's cooperation. TEE demonstrated severe eccentric MR with medial commissural prolapse due to chordae rupture (A3-P3 commissure) with left ventricular dilatation, mild tricuspid regurgitation (Fig. 1).
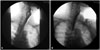
The patient complained of painful throat and odynophagia after TEE. The physical examination revealed tenderness and crepitus on right anterolateral area of neck (Level III) 3 hours later after TEE. Subcutaneous emphysema was detected on subsequent neck X-ray (Fig. 2A). Iatrogenic hypopharyngeal or esophageal injury was suspected, antibiotic treatment with piperacillin/tazobactam was initiated and the patient was not allowed to eat or drink. Computed tomography (CT) scan revealed subcutaneous emphysema without involvement of mediastinum, but the level of injury was not detected (Fig. 3). Esophagogram with gastrograffin swallowing showed no visible contrast leakage (Fig. 4A). Fiberoptic nasolaryngoscopic examination identified edema of the right posterolateral wall of the hypopharynx and hypopharyngeal bruise but there was no evidence of rupture or perforation. Intravenous antibiotic therapy was continued and nasogastric tube feeding was done. Laboratory analysis revealed an elevation of the white blood cell count (20.36 × 103/µL) and C-reactive protein (CRP; 28.54 mg/dL).
We tried to find any evidence of esophageal injury because treatment strategy would be different if the esophagus was involved. An ENT specialist and a GI specialist agreed with hypopharyngeal injury without esophageal damage after multiple tests. We concluded the lesion was limited to the hypopharynx because the presence of hematoma at the right side of hypopharynx, consistent with the direction and the depth of the probe passage. Further, there was no evidence of esophageal injury on serial follow-up multimodality imaging studies.
After 5 days from the injury, the subcutaneous emphysema disappeared and the patient remained afebrile with improvement of the leukocyte count and CRP (Fig. 2B). However painful neck mass around anterolateral area of neck was noticed (Level III). The follow-up CT without contrast showed a right parapharyngeal and retropharyngeal abscess secondary to hypopharyngeal injury (Fig. 5). Ultrasound guided needle aspiration was done for abscess drainage. Yellowish fluid in the abscess was analyzed for cytology and revealed as acute inflammatory cells predominantly neutrophils. As the patient's systemic status was stable with decrease of the leukocyte count and CRP, the antibiotics (piperacillin/tazobactam) was considered to be susceptible. The antibiotic treatment with piperacillin/tazobactam was maintained for 14 days with the drainage of abscess because no organisms were identified from the abscess fluid culture and repeated blood cultures.
On 7th day after TEE, second swallowing study was performed and no leakage was demonstrated (Fig. 4B), infectious parameters were continuously decreased, and follow-up fiberoptic nasolaryngoscopic examination demonstrated no evidence of perforation or rupture in hypopharyngeal cavity. So the patient was allowed to start eating small portions of soft food.
After 14 days of antibiotic therapy, when the infection was controlled completely, the patient had successful mitral valve repair with tricuspid annuloplasty with St. Jude Medical Tailor ring 31 mm.
Discussion
The overall incidence of severe hypopharyngeal and esophageal complications from traditional TEE is low.1)3)6) Risk factors of hypopharyngeal and upper gastrointestinal complications have been reported in few studies. Patient related risk factors include older age, short stature, presence of cervical spinal disease, chronic steroid use, presence of congestive heart failure.3)7)8) The presence of gastroesophageal pathology such as Zenker's diverticulum, esophageal stricture or obstructing mass, fibrosis secondary to prior chest radiation could be potential risk factor. Anatomical variation like massive cardiomegaly1)9) or tracheoesophageal fistula may be correlated to increase the risk.
Procedure related risk factors include inexperience of the cardiologist, and resistance to prove insertion with poor cooperation. To avoid direct injury to the hypopharynx and upper esophagus during a blind insertion of probe, appropriate conscious sedation and local anesthetic spray are recommended to lessen gag reflex and cricopharyngeal spasm. However, it is not always possible if the patient is not stable. Direct visualization of the passage of the probe with direct laryngoscope could be recommended to minimize blind injury of throat.
If there are procedural difficulties such as multiple attempts at passage of the TEE probe or resistance during insertion, the examination should be stopped. In addition, indirect injury is also result from increased continuous pressure on the probe positioned in the upper esophagus, therefore, the exam should be stopped if the resistance is continuing. Finally, it is very important to prevent sudden position change of the patient during the probe insertion. It needs pre-procedural enough education, adequate sedation, careful insertion of TEE probe, and an experienced assistant.
In our case, the patient had esophagogastroduodenoscopy previously in our hospital and had no anatomical anomaly. We assumed that the patient's poor cooperation and insufficient sedation might cause the wrong direction of the TEE probe and advancing force of TEE probe into the throat had led the probe to get lodged into the right pyriform sinus.
Treatment of hypopharyngeal perforation depends on the cause, timing of diagnosis, and type of lesion.101112) In a study of Hinojar et al.,10) 3 patients out of 7 patients were managed conservatively, whereas other 4 patients got surgical treatment. Mostly in the former cases, the time duration to the diagnosis was less than 1-2 days and involvement of infection was limited to pharyngeal space.
In current case, our patient complained pain in his throat and we detected subcutaneous emphysema within 3 hours after injury that may prevent aggravation of infection and lead good prognosis.
It is important not only to understand possible complications of the procedure and to recognize the risk factors of pharyngeal and esophageal injury, but also to detect the complication as soon as possible if it occurred, to get better prognosis.



 XML Download
XML Download