

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute myocardial infarction (AMI) is characterized by myocardial necrosis secondary to prolonged ischemia. Myocardial damage may lead to systolic and diastolic dysfunction, with the subsequent risk of left ventricular (LV) remodeling, neurohormonal activation, and vascular dysfunction.1) Ischemic injury after AMI affects not only systolic but also diastolic LV function. The phenomenon of myocardial stunning has also been shown to have both a systolic and a diastolic component.2) During the ischemic cascade, regional wall motion abnormalities appear early after the reduction in blood flow.3)4) Ischemia-induced diastolic dysfunction, or a delay in the onset of regional relaxation, has been demonstrated in the region perfused by the involved coronary artery in both animal and clinical models.5)6) LV diastolic dysfunction is an earlier, more sensitive sign of myocardial ischemia and persists longer than the systolic disturbance.7)8) The mechanism of diastolic dysfunction in patients with AMI may involve impaired diastolic relaxation, LV filling, or distensibility of the left ventricle, regardless of whether the LV ejection fraction (LVEF) is normal or abnormal.
For several decades, the recovery of LV systolic dysfunction after AMI and its prognostic implications have been the major focus of research. However, few studies have evaluated the impact of diastolic dysfunction on future clinical outcomes in patients with AMI in whom LV systolic function was preserved based on follow-up echocardiography. Therefore, the purpose of our study was to assess the role of diastolic functional recovery in predicting outcomes in such patients.
Methods
Study population
From August 2007 through July 2011, we identified a total of 2800 patients with AMI who underwent successful percutaneous coronary intervention at our institution. Among these, a total of 463 patients [mean age (± standard deviation) 63.2 ± 12.4 yr] who had preserved LV systolic function (defined as an LVEF greater than 50% on follow-up echocardiography at 6 months) were included in the final cohort. The patients were divided into two groups based on the presence or absence of diastolic functional recovery on echocardiography at 6 months after the index AMI: group I showed improvement (n = 241) and group II showed no improvement (n = 222). Improvement was defined as an increase of ≥ 1 grade in diastolic function on echocardiography at 6 months, as compared with the initial echocardiographic result. Improvement in the E/e' ratio (early filling/early diastolic mitral annular velocity ratio, as assessed by tissue Doppler imaging) from ≥ 10 on the baseline echocardiogram to < 10 at 6-month follow-up was also considered to represent improvement, regardless of diastolic functional grading (see Materials and Methods section). Non-improvement was defined as no change or worsening of diastolic function of ≥ 1 grade on 6-month follow-up echocardiography, as compared with the initial echocardiogram. The mean ages of groups I and II were 59.4 ± 12.2 and 67.3 ± 11.4 years, respectively, and there were 191 men in group I and 122 in group II. Major adverse cardiac events (MACE) included death, recurrent myocardial infarction (MI), and rehospitalization due to heart failure and were determined after the 6-month echocardiographic follow-up was completed. The study protocol was approved by the Institutional Review Board at our institution (2010-05-092).
Definitions of hypertension, diabetes, dyslipidemia, MI, and heart failure
Subjects were considered to have hypertension if their blood pressure was ≥ 140/≥ 90 mm Hg9) or if they were being treated for hypertension. The American Diabetes Association criteria10) were used to define diabetes mellitus: fasting plasma glucose levels ≥ 126 mg/dL on two consecutive assessments or if the patient was being treated for diabetes. Dyslipidemia was diagnosed according to the 2004 update of the NCEP guidelines.11) According to these guidelines, a high level of low-density lipoprotein cholesterol (≥ 160 mg/dL), a low level of high-density lipoprotein cholesterol (≤ 40 mg/dL), and a high level of triglycerides (≥ 150 mg/dL) were included in our assessment.12)
An MI with ST-segment elevation was diagnosed if the patient had continuous chest pain lasting more than 30 minutes, new ST-segment elevation ≥ 2 mm on at least two contiguous electrocardiographic leads, and a creatine kinase MB fraction (CK-MB) or troponin I (Tn-I) level greater than three times normal values.13) The presence of non-ST-segment elevation MI was diagnosed if the patient had chest pain without new ST-segment elevation and was positive for one of these cardiac biomarkers.14) Infarct-related arteries were identified using a combination of electrocardiographic findings, LV wall motion abnormalities on two-dimensional echocardiography, and coronary angiography.
A positive family history meant early cardiovascular disease in immediate relatives. Clinical demographic features were obtained from a review of hospital records.
Laboratory tests
Routine laboratory studies were obtained at the time of hospital admission. Cardiac enzymes, including CK-MB and Tn-I, were checked serially, and the maximal values were used in our data analysis. Blood samples to assess the serum lipid profile and glucose levels were obtained on the morning following admission. High-sensitivity C-reactive protein (hs-CRP) was measured by means of the immunoturbidimetric CRP-Latex (II) high-sensitive assay using an Olympus 5431 autoanalyzer (Olympus America Inc., Melville, NY, USA). Serum N-terminal pro-B-type natriuretic peptide (NT-proBNP) was measured using an electrochemiluminescence sandwich immunoassay method with an Elecsys 2010 analyzer (Roche Diagnostics, Mannheim, Germany), having an analytic range that extended from 5 to 35000 pg/mL.15)
Echocardiographic examinations
Two-dimensional, M-mode, and Doppler echocardiographic examinations were performed (Vivid 7, GE, Milwaukee, WI, USA), with the image point at the time of initial admission (day 1 or 2) and at 6 months after the MI. LV volume and EF were measured using Simpson's formula.16) The LV and left atrial (LA) volume indices were obtained by dividing volume by the body surface area. We used the mean values for three measurements taken by two independent observers of the technically-speaking "best" cardiac cycles from each examination. Intra-observer and inter-observer variabilities with Simpson's method were 4 ± 5% and 5 ± 4%, respectively (absolute difference divided by mean value of measurement).
The wall motion score index (WMSI) was derived for each patient. The left ventricle was divided according to a 17-segment model.17) For each segment, wall motion was scored from 1 (normal) to 4 (dyskinetic). Recordings were stored digitally and analyzed offline with EchoPAC PC software (GE Vingmed Ultrasound, Horten, Norway). All segments were assessed by means of strain rate imaging and wall motion score (WMS) on two-dimensional echocardiography, according to the American Society of Echocardiography guidelines. Because the number of infarcted segments per patient varied, WMSI was calculated as the average score for the segments studied in each patient.
Doppler echocardiograms were recorded on a strip chart recorder with a sweep speed of 100 mm/s. Early transmitral velocity (E wave) was measured by pulsed-wave Doppler from the apical four-chamber view, with the sample volume located at the tip of the mitral leaflets. Early diastolic (e'), late diastolic (a'), and systolic (s') velocities at the septal mitral annulus were obtained in this view by tissue Doppler imaging. LA volumes were measured using the multiple-discs method.18) The maximal LA volume was obtained before mitral valve opening and the minimal volume before valve closure. Volume measurements were averaged over three to five cycles. Diastolic dysfunction was considered normal, grade 1, grade 2, or grade 3 according to a multiparametric approach, including the E/A ratio, the E/e' ratio, and LA volume based on current guidelines.19) An elevated E/e' ratio and increased LA volume are associated with increased LV filling pressures.
Statistical analysis
The Statistical Package for Social Sciences for Windows, version 15.0 (SPSS Inc., Chicago, IL, USA) was used for all analyses. For each parameter, the mean, median, and standard deviation were calculated. Statistical significance between means for different groups was calculated by analysis of variance; statistical significance between frequencies was calculated by the chi-square test with Yates' correction or, if the expected value was less than 5, by Fisher's exact test. Relative risks (RR) and confidence intervals (CI) were also calculated. A p value of less than 0.05 was required to reject the null hypothesis. Variables found to be significant on the univariate analyses were entered into the multivariate models.
Results
Baseline clinical characteristics
Table 1 summarizes the baseline clinical characteristics for groups I and II. Patients in group II were older and included more women than the patients in group I, and hypertension and diabetes were more prevalent in group II. Prescribed medications did not differ between the groups except for the more frequent use of diuretics in group II (Table 2).
Laboratory, echocardiographic, and coronary angiographic findings
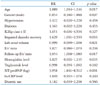
Table 3 summarizes the laboratory findings. Initial hemoglobin and triglyceride levels were lower, whereas the levels of NT-proBNP and hs-CRP were higher in group II than in group I. Echocardiographic findings are summarized in Table 4. The parameters used to assess diastolic function, such as LA size, LA volume, e', E/e', and E/e' at 6 months, were significantly more impaired in group II than in group I. Coronary angiographic findings, summarized in Table 5, showed no significant differences between the groups.
Clinical outcomes
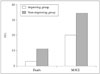
During the follow-up period (mean 910 ± 750 days), MACE occurred in 124 patients (31 deaths, 12 recurrent MIs, and 81 rehospitalizations due to heart failure) and were significantly more frequent in group II than in group I (76 vs. 48, respectively) (p = 0.001) (Fig. 1). Significantly more deaths occurred in group II than in group I (24 vs. 7, respectively) (p = 0.001), but the number of patients with recurrent MI (4 in group I vs. 8 in group II) as well as the number requiring rehospitalization (38 in group I vs. 43 in group II) did not differ significantly between groups I and IIII, 38. Cumulative survival and MACE-free survival rates were significantly lower in group II than in group I on Kaplan-Meier analysis (Fig. 2).
To identify independent predictors of mortality, we conducted a multivariate regression analysis using the variables of mortality found to be significant on univariate analysis. As shown in Table 6, age (RR = 1.089, CI = 1.044-1.136, p = 0.017), elevated NT-proBNP (RR = 3.958, CI = 1.841-8.512, p < 0.001), and impaired diastolic functional recovery (RR = 1.629, CI = 1.041-2.550, p = 0.033) were significant independent predictors of long-term mortality.
Discussion
The two main findings of this study are as follows:
1) Despite the recovery of LV systolic function after the index AMI, LV diastolic function had not improved by the 6-month follow-up in a significant proportion of patients.
2) Impaired diastolic functional recovery was an independent predictor of MACE after AMI.
AMI causes acute derangement of myocardial contraction and relaxation mechanics. In the case of myocardial ischemia, diastolic dysfunction often precedes systolic dysfunction. To overcome these abnormal changes, the myocardial repair process is activated immediately after an index AMI, and these dynamic processes are regulated by a number of cytokines and neurohormones to prevent progressive dilation of the left ventricle.20)21) Various factors such as interstitial edema, fibrocellular infiltration, and scar formation will also affect LV chamber stiffness,22)23) so many patients with AMI have a period of advanced diastolic dysfunction, as well as systolic dysfunction, after the acute episode.
Although acute diastolic and systolic dysfunction after AMI may improve with the successful restoration of coronary blood flow by means of a percutaneous coronary intervention, some patients show persistence or aggravation of systolic or diastolic functional abnormalities accompanied by chamber dilatation, so-called ventricular remodeling.24) Previous studies have shown that the persistent restrictive filling pattern at discharge may induce severe alterations in LV geometry or function, with a high risk for remodeling at 6 months,25) but the impact on clinical outcomes of impaired diastolic recovery during follow-up has been insufficiently evaluated.
In our study, diastolic function either did not improve or deteriorated in about a half the patients with AMI even though systolic function was found to be improved on echocardiographic follow-up at 6 months, and this persistent diastolic dysfunction was a significant predictor of long-term MACE. Therefore, our results suggest that serial monitoring of diastolic function would be useful in the risk stratification of patients with AMI, regardless of systolic functional status.
Diastolic function as evaluated on Doppler ultrasound provides important prognostic information that supplements information about systolic function.26)27) A previous meta-analysis of results from several prospective postinfarction clinical trials revealed that 20% of a large cohort of patients with AMI had restricted LV filling.28) Diastolic function was reversible, especially in patients with grade 3 and grade 4 diastolic dysfunction. However, Doppler variables can change rapidly and are affected by factors such as the patient's age, heart rate, and LV loading conditions, which explains why evaluating diastolic function with Doppler parameters alone is not sufficient. Because LA volume is less influenced by acute changes and reflects subacute or chronic diastolic function, it may be more reasonable to include LA volume status when assessing diastolic function in patients with AMI.29) In this study, we defined "improvement" in terms of grade of diastolic dysfunction and a decrease in the E/e' ratio to less than 10 at 6-month follow-up echocardiography, because patients with AMI reach a relatively steady state during this period of time.
The timing of echocardiography after infarction is critical in that LV chamber and myocardial stiffness may fluctuate before and after the repair process gets under way. The LV end-systolic volume index, LVEF, infarct size, and progressive ventricular remodeling are known to be predictors of clinical outcome after AMI. Although, as previously mentioned, risk stratification after AMI is often focused on LV systolic function, it appears that a more complete study of ventricular function that includes an assessment of LV diastolic function would be useful. In addition, significant LV diastolic dysfunction might persist despite an improvement in LV systolic function. Sustained LV diastolic dysfunction may have a significant impact on exercise capacity and long-term outcomes in patients treated with cardiac resynchronization therapy.30) The results of our study indicate that patients in whom persistent diastolic dysfunction persists after an AMI have a worse prognosis than patients whose diastolic function has recovered. Moreover, the prognostic information provided by a diastolic assessment is independent of that derived from an evaluation of systolic function alone.
There are several limitations in the present study. First, it is a retrospective observational study. Second, we did not consider the possible effects of risk factor modification that might influence clinical outcomes. Studies with longer follow-up periods are needed to determine such effects. Third, several factors that were not taken into account in the current analysis, such as coexisting illnesses, could also have affected LV diastolic function.
In conclusion, we found that the failure to recover LV diastolic function is not uncommon after AMI despite LV systolic functional recovery, and impaired diastolic function 6 months after an index AMI is a significant predictor of long-term clinical outcomes such as MACE. Therefore, serial monitoring of diastolic function over a period of at least 6 months would be useful in predicting future clinical adverse events in patients with AMI.






 XML Download
XML Download