

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Aortic regurgitation (AR) resulted by primary disease of the aortic valve leaflets and/or the wall of aortic root such as bicuspid aortic valve or rheumatic heart disease or secondary disease due to dilatation of ascending aorta such as degenerative change with hypertension or aortic dissection, etc. In contrast to acute AR, chronic AR may maintain normal left ventricular (LV) function through the combination of chamber dilatation with hypertrophy.
The conventional echocardiographic parameters such as left ventricular ejection fraction (LVEF) have limitations in predicting early LV dysfunction. Recent clinical studies have demonstrated changes in myocardial function through regional myocardial deformation imaging, including speckle-tracking echocardiography.1) We evaluated about prognostic value of myocardial longitudinal strain in patients with chronic AR.
Methods
This is single center non-randomized study and 314 patients with more than moderate chronic AR were enrolled retrospectively from January 2002 to December 2012. Following patients excluded: other significant valvular heart disease such as aortic stenosis or mitral disease, acute AR with infective endocarditis or aortic dissection, congenital heart disease, history of previous heart surgery and young age under 18 years old. Therefore, most pathogenesis of AR was degenerative change.
The grade of AR defined as Doppler parameters including visual estimated density (dense regurgitation flow on continuous Doppler), diastolic flow reversal in descending thoracic aorta (mid- to holo-diastolic) and jet deceleration time (pressure halt time less than 500 ms) and/or quantitative parameter including width of vena contracta (more than 0.3 cm), jet/left ventricular outflow tract width ratio (more than 45%) and regurgitation volume (more than 45 mL/beat).2)3)4) Patients didn't satisfied one or more those criteria were excluded.
All echocardiographic studies were performed using Vivid 7 machines (GE Vingmed Ultrasound AS, Horten, Norway). Measurement of LV dimension including LV end-diastolic diameter and LV end-systolic diameter was done with parasternal long axis image. LVEF, end-diastolic volume and end-systolic volume were measured using the biplane Simpson's method. Only apical four chamber images were used as strain rate data because of a number of patients' image couldn't be used due to poor image quality or too dilated LV cavity. Blinded offline analysis was performed using EchoPAC PC (GE Vingmed Ultrasound AS, Horten, Norway).
For continuous variables, a Student t test was performed for comparison between 2 groups. For categorical variables, the chi-square test or Fisher exact test were used for further analysis. The cutoff value of the myocardial longitudinal strain for the prediction of all-cause mortality was determined in receiver-operating characteristic (ROC) curve analysis as maximum sum of sensitivity and specificity. Survival according to baseline LV longitudinal strain of apical 4 chamber images (GS-4CH) was determined with use of the Kaplan-Meier method. We performed a multivariate Cox regression analysis to examine the association of the GS-4CH value and mortality of moderate or severe AR with or without aortic valve replacement (AVR). Statistical significance was assumed when the null hypothesis could be rejected at p < 0.05. Statistical analyses were conducted with SPSS version 20 for Windows (SPSS Inc., Chicago, IL, USA).
Results
The data of total of 60 patients with chronic AR was analyzed, finally. The severity of AR was assessed by mostly visual estimated density, jet deceleration time and diastolic flow reversal, severe AR were 28 (47%), moderate to severe AR were 24 (40%) and moderate AR were 8 (13%) on the initial echocardiogram. During about 64 months follow-up period (median 63.87 ± 33.2 months; range 1 day-10.2 years), 38 patients (63%) underwent AVR and 16 patients (27%) were deceased. The most causes of death were cardiovascular death [sudden cardiac death (n = 3), heart failure (n = 3)] and acute cerebral accident (n = 2) in mainly who received conservative treatment (n = 7 vs. 1). The mean age was 55 years (range 24-82) and 61.7% was male. The mechanism of AR was mostly degenerative change, 9 patients (15%) had combined dilated ascending aorta (diameter more than 5.7 cm) and 1 patient had right coronary cusp tear probably related Behcets' disease. Acute AR patients who related aortic dissection or infective endocarditis were excluded when screening.
The deceased group was significantly older (69 ± 12 years old vs. 51 ± 17 years old, p < 0.001), more thin [body surface area (BSA) 1.46 ± 0.20 kg/m2 vs. 1.70 ± 0.19 kg/m2, p < 0.001], higher blood urea nitrogen (BUN) level (25.28 ± 12.84 mg/dL vs. 17.72 ± 6.63 mg/dL, p = 0.038) and fewer had AVR [5 patients (31.3%) vs. 33 patients (75.0%), p = 0.005]. The history of atrial fibrillation was more frequent in deceased group [5 patients (31.3%) vs. 2 patients (4.5%), p = 0.012]. However, incidence of other past history including hypertension, diabetes, hyperlipidemia, ischemic heart disease (IHD) and chronic renal failure was not significantly different between two groups. In aspect of two-dimensional echocardiographic parameters, deceased group had more decreased LV function (LVEF 42.9 ± 13.4% vs. 49.8 ± 11.2%, p = 0.050), increased E/E' ratio (18.3 ± 9.1 vs. 12.3 ± 6.1, p = 0.028), and decreased GS-4CH value (-12.1 ± 3.7% vs. -15.7 ± 4.4%, p = 0.005) (Table 1).
The patients who received AVR (AVR group) were younger than patients who received conservative treatment (conservative group) (51.8 ± 14.7 years old vs. 61.9 ± 20.8 years old, p = 0.053). In AVR group, the patients had bigger body surface area (1.70 ± 0.19 kg/m2 vs. 1.53 ± 0.22 kg/m2, p = 0.002), lower BUN level (17.96 ± 8.11 mg/dL vs. 23.06 ± 10.58 mg/dL, p = 0.046) and lower mortality [5 patients (13.2%) vs. 11 patients (50.0%), p = 0.005] than conservative group. The mean follow-up duration was longer in AVR group than conservative treatment group (40 ± 29 months vs. 71 ± 30 months, p < 0.001). Otherwise, there was no significant difference between the two groups (Table 2).
Decision of surgery often depended on demographic factor such as age, tendency of physician or will of the patient or the family rather than classical operative indication. The 5 (13.2%) of 38 patients who received AVR were not correspond with indication, while 18 (81.8%) of 22 patients who received conservative management although appropriate with surgical indication. The most common causes of deferred surgery were patient's refusal (n = 8, 44%) and withholding of physicians due to old age or poor condition (n = 6, 33%) (Fig. 1).
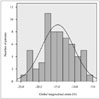
The median value of longitudinal GS-4CH was -14.70 ± 4.46% (range -23.9--6.3%, frame rate 34.63 ± 14.31/sec, heart rate 74 ± 16 bpm) (Fig. 2). In ROC curve for mortality of patients with chronic AR, classical markers such as LVEF or LV dimension didn't show significant predicting power [area under the curve (AUC) 0.360 vs. 0.425]. On the contrary, global longitudinal strain representing as GS-4CH has impact to mortality of chronic AR and the most powerful predicting level was -12.5% (sensitivity 0.688, specificity 0.795, AUC 0.744) (Fig. 3). In AVR group, GS-4CH was more predictive than conservative group (AUC 0.894 vs. 0.682).
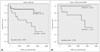
In cumulative survival curves using Kaplan-Meier method, patients with decreased GS-4CH value (> -12.5%) showed significantly increased mortality (log rank p = 0.001) (Fig. 4). In decreased GS-4CH group, the patients were older (64 ± 13 years old vs. 51 ± 18 years old, p = 0.002) and thin (BSA 1.56 ± 0.22 kg/m2 vs. 1.68 ± 0.21 kg/m2, p = 0.039). They had more frequently previous IHD (4 patients, 20% vs. 1 patient, 2.5%, p = 0.038) and lower LVEF (38.60 ± 12.37 vs. 52.58 ± 8.92, p < 0.001). However, other manifestations such as sex, comorbidity and laboratory finding didn't show significant difference between low and high GS-4CH group (Table 3).
On multivariate analysis by Cox proportional hazard model adjusting for age, sex, BSA, past history of atrial fibrillation, level of BUN, LVEF, LV dilatation and AVR, decreased global longitudinal strain rate on apical four chamber image proved to be an independent predictor of all-cause mortality in patient with chronic AR (hazard ratio 1.313, 95% confidence interval 1.010-1.706, p = 0.042) (Table 4).
Discussion
In chronic AR, adaptation to increased preload and afterload results in increase in end-diastolic volume with eccentric and concentric hypertrophy. LV hypertrophy inhibits the increase of wall stress and it enable to maintain normal LVEFs and asymptomatic state for considerable period. According to AR persist, the wall thickening fails to cope the hemodynamic overload and systolic function insidiously decreased. In this stage, symptom such as dyspnea or exertional chest pain may represent, and some patients remained asymptomatic until severe LV dysfunction has developed. Ten-year survival rate was 69 ± 9% and cardiac event free survival rate was 37 ± 8% in asymptomatic patients with even severe AR in study of Detaint et al.5)
In natural history of AR, progression to symptoms and/or LV dysfunction is less than 6% per year among asymptomatic patients with normal LV systolic function. Whereas, greater than 25% per year of asymptomatic patients with LV dysfunction progress to cardiac symptoms and the mortality rate of symptomatic patients is greater than 10% per year.2)6)
LV systolic dysfunction is initially reversible and it is possible to fully recovery of LV size and function with AVR. The classic indications for valve replacement are development of symptom such as dyspnea more than NYHA class 3, LV dysfunction (LVEF < 50%) or dilated LV dimension (LV end diastolic dimension > 75 mm or end-systolic dimension > 55 mm).2) However, there is no single parameter to detect this period and the timing of AVR in patient with chronic AR is still debated. And once myocardial dysfunction developed, it could cause high risk for post-operative heart failure and death.
The factors predictive of reduced postoperative survival and recovery of LV function in patients with AR are severity of preoperative symptoms or reduced exercise tolerance, severity of depression of LVEF and duration of preoperative LV systolic dysfunction.2) Tornos et al.7) studied about 101 patients with asymptomatic chronic AR and normal LVEF for up to 10 years. During the follow-up period, 14 patients needed surgery (8 patients because of symptoms and 6 patients because of LV impairment), baseline end-systolic diameter > 50 mm and LVEF < 60% were independent predictors for cardiac symptoms or LV dysfunction.7)
Guideline recommendations for AVR have focused on LVEF and LV end systolic dimension as measures of LV pump performance, and LV end-diastolic dimension as a measure of the severity of the volume overload.2)
In volume overloading state such as chronic AR, it tends to overestimate LV systolic function. The conventional echocardiographic parameters such as LV dimensions and the LVEF have limitation in predicting early LV dysfunction, thus recently many studies investigated about quantitative measurement of LV function used speckle-tracking echocardiography. Myocardial strain rate imaging derived from tissue Doppler echocardiography estimates spatial gradients of myocardial velocities and allow accurate quantification of regional myocardial function, therefore it facilitate early detection of subclinical myocardial disease.8)9)10)11) Another study about myocardial deformation in 59 asymptomatic patients with isolated wide range of severity of AR showed that strain rate imaging is a sensitive tool in detecting changes of contractility.12)
Di Salvo et al.13) studied about asymptomatic 26 patients aged ≤ 16 years with isolated moderate to severe AR. The patients were divided to stable and progressive AR (defined as development of symptoms, increased LV volume more than 15%, or decreased LVEF more than 10% during follow-up) group. In patients with progressive AR group, LV average longitudinal strain was significantly reduced (-17.8 ± 3.9% vs. -22.7 ± 2.7%, p = 0.001) although baseline LVEF was similar. Among echocardiographic parameters including LV end diastolic dimension and LV volume, E/E' ratio and jet area/LV outflow tract area ratio, LV average longitudinal strain was only significant risk factor for progressive AR (cut-off value > -19.5%, sensitivity 77.8%, specificity 94.1%, AUC 0.889).13)
Olsen et al.14) performed longitudinal study in 64 patients with moderate to severe AR and demonstrated that reduced myocardial systolic strain was associated with disease progression during conservative management and impaired outcome after surgery. The present study showed no significant different echocardiographic findings including LVEF, LV dimension and GS-4CH between conservative and AVR group. In AVR group (n = 38), 5 patients (13%) were deceased and they had significant lower GS-4CH level (-9.02 ± 1.64% vs. -15.46 ± 4.42%, p = 0.003; AUC 0.897) although LVEF and LV end-diastolic dimension weren't (43.40 ± 16.79% vs. 50.06 ± 10.83%, p = 0.241; AUC 0.397, and 6.26 ± 1.74 cm vs. 6.40 ± 0.85 cm, p = 0.865; AUC 0.539). In conservative group, deceased patients were 11 (50%), GS-4CH didn't show significant difference between survivors and deceased patients in common with LVEF and dimension.
In these days, speckle-tracking deformation imaging has become routine echocardiographic examination. Echocardiographic analysis of LV longitudinal strain rate with speckle-tracking echocardiography is useful to early detect LV dysfunction and determine the right timing of operative management in patients with chronic, isolated AR. Measurement of GS-4CH is easier and faster than global longitudinal strain because it is possible with apical 4 chamber image alone. And the present study showed GS-4CH has sufficient predicting value for mortality in patients with chronic aortic regurgitation. GS-4CH may be a simple and useful surrogate marker in predicting the fate of chronic AR.
Limitations
This number of enrolled patients was small because it is based on single center data and isolated chronic AR without other valvular heart disease is not common. The follow-up duration of patients was very various (1 day-123 months, mean 60 ± 33 months) and moreover, there are lack of information about mechanism of AR, concomitant coronary artery disease and medical treatment. Few patients had done cardiac catheterization and/or coronary angiography. We assumed etiology of most patients is degenerative change as echocardiographic findings. Because of some patients' LV chambers were so dilated and frame rates were lower than optimal range, data collection for strain measurement was limited. Further evaluation with global circumferential and radial strain may strengthen predicting power to prognosis of patients with chronic AR.
Conclusions
In this study, global strain represent as GS-4CH had independently significant predictive value for all-cause mortality after adjusting for other affecting variables while conventional parameter such as LVEF or LV dimension did not. GS-4CH seems to be useful parameters to support decision making and predict prognosis in patients with chronic AR.






 XML Download
XML Download