

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sinus of Valsalva aneurysms, rare cardiac anomaly, are most often caused by weakness at the junction of the aortic media and the annulus fibrosus.1) Ruptured sinus of Valsalva aneurysms (RSVA) are frequently associated with other congenital defects, particularly with ventricular septal defect (VSD) and, aortic regurgitation (AR). The principal VSD associated with a RSVA is supracristal type.2)3)4) The supracristal VSD is the predominant type reported in Asian countries, whereas the perimembranous VSD is often seen in Western countries.5)6) Membranous septal aneurysms are bulging of the membranous portion of the interventricular septum below the aortic annulus in the right ventricle (RV). Sinus of Valsalva aneurysms must be distinguished from membranous septal aneurysms. However, sometimes it is difficult to differentiate the two because they occur anatomically adjacent to each other at the level of aortic annulus. Here, we report a case of sinus of Valsalva aneurysm mimicking membranous septal aneurysm associated with perimembranous VSD, that was ruptured later, causing severe right-sided heart failure.
Case
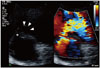
A 20-year-old man visited our clinic for an evaluation of exertional chest pain. The patient had a history of VSD which had been seen at neonate. He had been checked regularly without events until the time of his presentation. Transthoracic echocardiography (TTE) and exercise treadmill test were performed. At parasternal short axis view, perimembranous VSD was detected with color Doppler imaging. There was a suspicious focal aneurysmal dilatation around the defect (Fig. 1, Supplementary movie 1 and 2). Left ventricular (LV) end-diastolic and end-systolic dimension were 52 mm and 31 mm, respectively. Qp/Qs was 1.2. Initially, these findings were considered clinically insignificant membranous septal aneurysm. The exercise treadmill test was negative. The patient was scheduled for a regular follow-up. However, the follow-up was lost. Four years later, the patient visited emergency room due to nausea and vomiting lasting for one month. Continuous murmur is auscultated at left parasternal region. Mild pitting edema is presented at both lower legs. Abdomen computed tomography showed ascites and cutaneous edema without any evidence of cirrhosis of the liver, raising the possibility of right-sided heart failure. TTE showed enlargement of RV combined with depressed function. The LV was enlarged but the function of LV was preserved (Supplementary movie 3). However, the interventricular septum was flattened toward LV. At parasternal view, the width of VSD was wider than the width shown in the previous study (Supplementary movie 4). Color Doppler imaging showed turbulent systolic jet with a large proximal isovelocity surface area through the defect (Fig. 2C, Supplementary movie 5). There was definitely an elongated aneurysm of the right sinus of Valsalva with the tip ruptured (Fig. 2A, B, and C, Supplementary movie 6). Fortunately, the aortic valve had normal morphology without aortic regurgitation (Supplementary movie 7). Continuous wave Doppler revealed the diastolic jet flow from the aortic root to the RV through the ruptured aneurysm and systolic jet flow through VSD (Fig. 2D). The patient was referred to the department of cardiac surgery for open heart surgery. After median sternotomy, enlarged RV and prominent appendage of right atrium was observed. Aortotomy revealed ruptured aneurysm with windsock appearance which was closed with Dacron patch (Fig. 3A). However, the aortic valve was normal and left untouched. Subsequent right ventriculotomy exposed the perimembranous VSD sized about 1 cm which was also closed with Dacron patch (Fig. 3B). The weaning of cardiopulmonary bypass pump was successful. Postoperative course was uneventful. Follow-up echocardiogram after one year showed no evidence of residual shunt or AR and showed normalization of LV and RV size. The functions of both ventricles were well preserved.
Discussion
Sinus of Valsalva aneurysms are very rare, with incidence rate ranging from 0.1% to 3.5% of all congenital heart diseases.7) Sinus of Valsalva aneurysms occur three times more often in males, with the highest incidence in Asian populations.8) Most sinus of Valsalva aneurysms arise from the right or the noncoronary sinuses. They commonly rupture into the RV or right atrium.
VSD and AR are frequently associated with RSVAs. The incidence rate of associated aortic sinus aneurysms and VSD ranges from 34.6% to 82.4%, with higher rate in Asian countries, including Korea.3)4)8)9)10)11)12) Principal VSD associated with RSVA is supracristal type.2)3)4) Supracristal VSD is the predominant type seen in Asian countries, whereas perimembranous VSD is often seen in Western countries.5)6) In the present case, RSVA was associated with perimembranous VSD which was suspected on echocardiography based on the 11 o'clock direction of shunt flow, which was confirmed by the surgeon. The size of VSD was larger than measured with TTE. This could be due to the shape of VSD that was ovoid, which might have induced error in the measuring of the defect size. In patients with asymmetric defects like the present case, real-time three-dimensional echocardiography is a complementary tool to assess the size and morphology of defects more accurately.13)
The incidence rate of associated sinus of Valsalva aneurysm and AR ranges from 20% to 64.7%.3)8)11) It is well known that supracristal VSD is the preceding pathology.11) Anatomically, most sinus of Valsalva aneurysms are congenital in origin, caused by the lack of fusion between the media of the aorta and the annulus fibrosus of the aortic valve.1) Hemodynamically, the flow through VSD produces Venturi effect, a tendency for the related aortic sinus and cusp to pull away from closure. These two mechanisms induce AR, and AR begets AR. Surgical treatment of AR in addition to repairing the RSVA is needed in some patients. The incidence of associated perimembranous VSD and AR is 2.4 times less common compared to that of associated supracristal VSD and AR.14) Eapen et al.15) suggested echocardiographic features of perimembranous VSD susceptible to AR, presence of aortic cusp override, aortic cusp movement abnormalities, and presence of color flow mapping across ventricular septum. In the present case, the perimembranous VSD was not associated with AR. There was no finding of aortic cusp override or aortic cusp movement abnormality, decreasing the possibility of associated AR despite the strong jet flow across ventricular septum.
Echocardiography is necessary for the definitive diagnosis. The accuracy of TTE is about 75%.16) TTE shows the site and size of aneurysm, the direction of the rupture, which helped us find the associated VSD, fluttering of tricuspid valve, and shunt flow.16)17) In case TTE fails to show the accurate anatomical structure, transesophageal echocardiography (TEE) images of various angles such as RV outflow tract, sinus of Valsalva and aortic root, and color Doppler help us assess the exact flow velocity and direction through RSVA or VSD.18)
The membranous septal aneurysms are bulging of the membranous portion of the interventricular septum below the aortic annulus in the RV. Membranous septal aneurysms, associated with VSD in 19% of cases,19) play a role of spontaneous VSD closure in children. Sinus of Valsalva aneurysms must be distinguished from membranous septal aneurysms because these two distinct pathologies lead to different results. Sinus of Valsalva aneurysm leads to rupture causing serious symptoms like the current case, whereas membranous septal aneurysms lead to spontaneous VSD closure in selected cases, especially in children.20) However, these two distinct pathologies sometimes are difficult to differentiate, especially in poor echo window, because they occur anatomically adjacent to each other at the level of aortic annulus. Sinus of Valsalva aneurysms are located above the aortic annulus (Fig. 4A), whereas membranous septal aneurysms are located below the annulus (Fig. 4B). Therefore, multiple views are helpful to differentiate these two pathologies. With only a single image at the parasternal short axis view, it is difficult to differentiate whether the aneurysm is located above or below the annulus. In the present case, at initial exam, the operator rashly concluded that the focal aneurysm around the VSD was membranous septal aneurysm based on the parasternal short axis view. If the operator had a close look at the aneurysm on multiple views, the aneurysm would have been found to be located above the annulus, the diagnosis would have changed.
In conclusion, in young patients with unexplained chest pain, sinus of Valsalva aneurysm could be suspected. Echocardiography should be performed. Careful TTE with multiple windows and TEE in selected cases are needed to confirm the diagnosis. Sinus of Valsalva aneurysms should be differentiated from membranous septal aneurysms because these two pathologies occur anatomically adjacent to each other at the level of aortic annulus. Unruptured or ruptured sinus of Valsalva aneurysms with VSD should be repaired surgically as early as possible. Before going to the operating room, it should be determined whether AR is present. If AR is present, surgical treatment of AR in addition to repairing the RSVA is needed.



 XML Download
XML Download