

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A 25-year-old man was evaluated due to progressive exercise intolerance and desaturation in the setting of previously documented Tetralogy of Fallot (TOF). He was diagnosed with TOF shortly after birth but his family declined surgery. Three years earlier, he had undergone left sided modified Blalock-Taussig shunt as a palliative procedure due to progressive shortness of breath and desaturation (O2 saturation between 80-85%). Initially, in the first few months after the procedure, he noticed slight improvement of his symptoms. However, he developed progressive exercise intolerance and desaturation which mandated complete repair. Physical examination was remarkable for desaturation (O2 saturation between 85-90%), clubbing and systolic ejection murmur (grade II-III/VI) over the pulmonic area. Electrocardiogram showed right axis deviation and right ventricular (RV) hypertrophy. Chest X-ray revealed dilated right side of the heart.
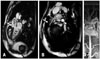
Transthoracic echocardiogram (TTE) was technically difficult still showed dilated hypertrophied RV with normal systolic function, malalignment ventricular septal defect (VSD) and overriding of the aorta (Supplementary movie 1 and 2). Transesophageal echocardiogram (TEE) was carried out for further delineation of the RV outflow tract (RVOT) which was hypoplastic with a long (~4 cm) segment of narrowing and significant infundibular narrowing (by hypertrophied muscle bundle). Peak gradient across the RVOT was approximately 35-40 mm Hg (Fig. 1, Supplementary movie 3 and 4). Cardiac magnetic resonance (CMR) was technically challenging due to patient's non-compliance with breathing instructions, yet confirmed the findings of TTE/TEE. Additionally, CMR uncovered hypoplastic proximal main pulmonary artery (PA), dilated left PA and mild proximal right PA stenosis with hypoplasia throughout the course (Fig. 2, Supplementary movie 5). The patient underwent successful complete repair with RV to PA conduit, resection of the native RVOT muscle bundles, arterioplasty of the right PA and VSD pericardial patch closure. Surgery was uneventful.

 XML Download
XML Download