

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiac involvement in hypereosinophilia is rare; when present, its various manifestations range from heart failure to thromboembolic events and/or atrial fibrillation, which are caused by fibrous thickening of the endocardium of one or both ventricles and mural thrombosis.1)2)
Toxocara canis (T. canis) is a common roundworm in dogs. Toxocariasis with concomitant eosinophilia is an often asymptomatic and self-resolving condition; however, clinical forms of toxocariasis may be present.3) Myocarditis occurs in 10-15% of cases of visceral larva migrans, and in those cases, myocarditis is accompanied by an increased level of circulating eosinophils.3) Here, we report a patient who presented with right heart failure, a thickened right ventricular apex with thrombus, and peripheral eosinophilia for 8 months, which was associated with toxocariasis.
Case
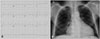
A 57-year-old male presented to the hospital with generalized edema and recently progressive dyspnea. He had been treated at an outside hospital after presenting with a pericardial effusion, right atrium (RA) thrombus, and ascites for 2 months. The patient was a farmer who owned a dog. When he visited the hospital, his vital signs were stable with blood pressure, 130/80 mm Hg; pulse rate, 98 beat/min; respiratory rate, 20 breaths/min; and body temperature, 36.4℃. Physical examination revealed jugular venous distension in the sitting position, decreased breaths sound in the bilateral lower lung fields, a severely distended abdomen with shifting dullness on percussion, and pretibial pitting edema. Cardiac auscultation revealed a grade 2/6 systolic heart murmur, and electrocardiography demonstrated atrial flutter with a ventricular rate of 77 bpm (Fig. 1A). Laboratory findings included an elevated cardiac troponin I level of 59 ng/L (normal range, 0-40 ng/L), mildly elevated liver enzymes (direct bilirubin 0.71 mg/dL, alkaline phosphatase 223 IU/L), and a high-sensitivity C-reactive protein of 7.12 mg/dL (normal level 0-0.75). Complete blood count showed a white blood count of 9.4 × 109/L with 15% eosinophils (1410/mm3), and eosinophilia was persistent since 8 months ago from the past medical records. Metabolic profile and urinalysis were normal. A chest radiograph showed cardiomegaly and blunting of the bilateral costophrenic angles (Fig. 1B). Transthoracic echocardiography showed an enlarged RA with spontaneous echo contrast, no definite thrombus, and a normal left ventricular ejection fraction (Fig. 2). There was a moderate pericardial effusion (Fig. 3A, Supplementary movie 1) and moderate tricuspid regurgitation with an elevated right ventricle (RV) systolic pressure (49 mm Hg). Interestingly, dense RV apical trabeculations with a large hypoechogenic mass occupied the apex (Fig. 3B, Supplementary movie 2), highly suggestive of a free floating thrombus. After review of previous echocardiography at the outside hospital, we identified that this RV apical mass was present for at least 3 months (Fig. 4A) and associated with an RA thrombus (Fig. 4B), which disappeared after anticoagulation. Pericardiotomy was performed, and biopsy revealed non-specific pericarditis without evidence of tuberculosis. After pericardiostomy, pericardial effusion was disappeared (Fig. 5A) without alteration of the dense RV apical mass (Fig. 5B, Supplementary movie 3).
Chest computerized tomography showed no pulmonary thromboembolism, a normal endobronchial lesion, and normal coronary arteries with a relatively hypodense thickened RV apical endomyocardium, suggesting RV apical fibrosis with thrombus (Fig. 6A). A cardiac manifestation associated with hypereosinophilia was suspected based on echocardiographic findings with a suspicious RV apical thrombus and peripheral eosinophilia.4) Further work-up the following day with cardiac magnetic resonance imaging (MRI) showed thickening of the hypodense RV apex (Fig. 6B) with delayed enhancement after administration of gadolinium (Fig. 6C), suggesting an RV apical thrombus with endomyocardial fibrosis or inflammation.
We performed an endomyocardial biopsy and serological studies in order to define the cause of the patient's eosinophilia and symptoms; however, endomyocardial biopsy showed no evidence of eosinophilic infiltration. There was elevation of Ig G (2000 mg/dL; normal range, 650-1500 mg/dL) and a greater elevation of total Ig E (5000 IU/mL; normal range, 0-380 IU/mL). Through further work-up, we excluded secondary hypereosinophilia (due to malignant diseases, allergy, vasculitis, parasitic infection). Since the initial tests were inconclusive and the patient had a history of occupational canine exposure, serological tests for parasites were done. The diagnosis of toxocariasis was confirmed by serological exams [ELISA for T. canis positive; 2.306 (cut off: 0.848)]. He was treated with anticoagulation by intravenous infusion of unfractionated heparin, which was later bridged to warfarin. In addition, intravenous furosemide (20-40 mg/day) was administered to control ascites and edema. Since the patient's symptoms were relieved by management of his heart failure, immunosuppressive treatment was not initiated. In addition, due to clinical and laboratory improvement, he was not treated with albendazole.
Discussion
Hypereosinophilic syndrome is a rare condition, consisting of an elevated persistent eosinophil blood count (> 1500 cells/mm3 for at least 6 months) and evidence of organ dysfunction related to eosinophil infiltration.5) Cardiac involvement, generally affecting the myocardium, is noted in more than 50% of patients. Presentations include either right or left ventricular effects, pericardial or global myocardial manifestations, heart failure, intracardiac thrombi, myocardial ischemia, arrhythmias, or pericarditis.2)5) During the early necrotic stage, eosinophil infiltration produces endocardial microabscesses, and subsequently a thrombus is formed on the surfaces of the myocardium of both ventricles. Finally, endomyocardial fibrosis occurs with congestive heart failure;6) Loeffler's endocarditis is thought to be a late cardiac manifestation that is characterized by fibrous thickening of the ventricular endocardium with extensive eosinophilic infiltration leading to apical thrombotic obliteration.4)7)8) Endomyocardial biopsy is currently the gold standard for diagnosis, although typical findings from noninvasive methods such as cardiac MRI may suggest the diagnosis. In the present study, MRI and endomyocardial biopsy yielded non-specific findings.
Toxocariasis associated eosinophilia is often asymptomatic, but the various clinical forms of toxocariasis may be present.3) When infectious eggs of T. canis reach the human gastrointestinal tract, they enter the portal system and the liver. Following this, some visceral larva migrate from the liver to various organ systems such as the skin, lungs, and on rare occasions, the heart and central nervous system through the systemic circulation. Loeffler's endomyocarditis and pericardial tamponade are the unusual manifestations described in the literature.9)10) Although there was no evidence of eosinophilic infiltration in the endomyocardial biopsy, considering possibility of inadequate tissue due to thrombus or fibrosis, we hypothesized that the cardiac manifestations in our patient were due to eosinophilic infiltration and that the myocardial damage increased troponin levels. Our patient had a diagnosis of toxocariasis with myocardial manifestations, along with generalized symptoms and eosinophilia for 8 months. Other diseases accompanied by eosinophilia were ruled out. The diagnosis was confirmed with serological tests (ELISA) for T. canis. The combination of serological tests, clinical manifestations, laboratory findings, and the patient's occupational history supported the diagnosis. The patient remains on drug therapy, and serial follow-up echocardiography is also planned.
Until now, we have not been able to find any reports of RV involvement from hypereosinophilia caused by T. canis. Our case suggests that when a patient who has myocarditis with eosinophilia presents, toxocara infection should be considered as a possible cause of eosinophilia, especially when there is a history of exposure to dogs and when the patient is a professional dog trainer.





 XML Download
XML Download