

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atrial septal defect (ASD) is a common congenital heart defect that constitutes 7.5-10% of all congenital heart defects found in children,1)2) and is one of the most common congenital heart lesions presenting in adult life.3) The hemodynamic mechanism of ASD is a left-to-right shunt, which induces a volume overload to the right ventricle (RV). Although this volume overload can be well tolerated,4) if it is sustained it can be detrimental and can cause adverse outcomes.5)6) During follow up of patients with ASD, functional parameters that are able to detect subtle changes in RV function are needed to evaluate the status of patients.
Myocardial deformation imaging techniques have recently been developed to measure strain (є) and strain rate (SR). These parameters are closely related to the intrinsic function of the myocardium,7) and are relatively independent of myocardial loading.8)9) Analyses of є and SR values have been performed in other illnesses affecting the RV10)11)12)13) and in ASD.14)15)16)17)18)19)20)
In ASD patients, no differences have been found between pre- and post-closure RV deformation values determined at the mid-segment of the RV free wall.14)15) However, more recent studies have applied a segmental analysis approach and divided the RV free wall into two or three segments.16)17)18)20) In ASD patients prior to defect closure, RV apical є and SR were higher than in controls,16)17)20) and these values decreased after defect closure.16)18)20) These results suggest that in patients with ASD, the deformation of the RV apical segment is dependent on the loading of the RV.
Studies analyzing RV deformation in ASD patients are often limited by the small number of available subjects, and the lack of an analysis method to assess the correlation between deformation values and parameters that are linked to RV loading, measured using cardiac catheterization.14)15)16)17)18)19)20) This study aims to identify the dependence of the RV free wall longitudinal deformation on RV loading, by examination of the apical and basal segments of the RV free wall in a relatively large number of ASD patients.
Methods
Between March 2009 and December 2012, 146 children with ASD were admitted to the Department of Pediatrics, Asan Medical Center, Korea, for percutaneous device closure of defect. One hundred fourteen among them had qualified for echocardiographic images to analyze RV free wall deformation before and after device closure and also had complete results from catheterization studies, and so were enrolled as subjects in the present study. Five patients with major cardiac anomalies and 27 patients with incomplete echocardiographic image data were excluded. As a control group, 60 age matched healthy children were enrolled. These children had been referred for evaluation of a heart murmur or for nonspecific chest pain during the aforementioned period, and clinical and echocardiographic examinations had shown no evidence of cardiac disease. There were no additional cardiac anomalies in patients, except for one patient with persistent left superior vena cava. Associated systemic problems were Down syndrome in two patients, CATCH22 in one patient, and Kallmann syndrome in one patient. The institutional review boards of the Asan Medical Center approved this retrospective study (2013-0614) and waived the need for patient consent.
Echocardiographic examination
Echocardiographic examinations were performed both the day before and within 24 hours of the percutaneous closure of defects in 114 subjects with ASD. The subjects were prepared for examination in the left lateral decubitus position and a sedative (chloral hydrate) was administered as required. An iE33 (Philips, Bothell, WA, USA) equipped with a 5-MHz transducer was used. Still images from subcostal, apical and parasternal views, and moving images from modified apical four-chamber view (3 cardiac cycles, 61-72 frames/s) were stored.
All offline measurements were performed by one author blinded to the demographic and catheterization data of the subjects. Two dimensional (2D) measurements were performed using Image-Arena version 4.6 (TomTec Imaging Systems, Unterschleissheim, Germany). RV longitudinal dimension (RVLD) was measured according to the guidelines of the American Society of Echocardiography,8) and indexed RV longitudinal dimension (iRVLD) by division with the body surface area which was calculated using the Haycock formula.21)
Two segment analyses of RV free wall deformation
Analyses were performed using a 2D Cardiac Performance Analysis Version 1.2.3 (TomTec Imaging Systems, Unterschleissheim, Germany) by the single examiner. Longitudinal systolic є and SR were measured from the stored moving images of the modified apical four-chamber view, using a two segmental approach, following the structure of the RV free wall with a smooth inlet and trabeculated apex, as has been described previously.10)16) The left ventricular algorithm was applied to the RV. The endocardial border was manually traced at end diastole starting from the tricuspid annulus to the RV apex (Fig. 1A). Tracking was performed automatically. Values of є and SR were obtained at two points, which were selected as the middle positions of the respective basal (єB, SRB) and apical (єA, SRA) segments (Fig. 1B). The values from the best tracked cycle out of three were selected as the data to be used for analysis, and were converted to absolute values.
To account for the decrease in the RV deformation seen in a bigger ventricle, we adjusted the deformation values to the longitudinal RV length, according to the approach by Dragulescu et al.17) However, we substituted iRVLD for RVLD in this adjustment to avoid an overestimation of the resultant values in older subjects. We think that iRVLD is more appropriate than RVLD which should be dependent on the growth of children, not only dependent on a remodeling from the volume overload. In detail, RV longitudinal length adjusted deformation indexes were calculated by multiplying values of є and SR with iRVLD as єBL = єB × iRVLD; єAL = єA × iRVLD; SRBL = SRB × iRVLD; SRAL = SRA × iRVLD.
We randomly selected 16 subjects to determine the intra- and inter-observer variability in the deformation value measurements. The deformation values were measured by one observer on two occasions and by two observers on two occasions, and the percent precisions were calculated.22) The percent precision of intra-observer for єB, єA, SRB, and SRA measurements was 3.7%, 4.1%, 7.4%, and 8.9%, respectively; the percent precision of inter-observer was 8.5%, 7.2%, 13.7%, and 6.6%, respectively.
Cardiac catheterization
Cardiac catheterization was done under general anesthesia. In all ASD patients prior to defect closure, mean pulmonary arterial pressure and RV end diastolic pressure (RVEDP) had been measured. Pulmonary to systemic flow ratios (Qp/Qs) were calculated, according to Fick's principle. These catheterization results were used as independent variables in the analyses of the deformation values.
Defects were successfully closed by an insertion of an appropriately selected Amplatzer Septal Occluder (AGA Medical Corporation, Golden Valley, MN, USA).
Statistics
All numerical data are presented as means ± standard deviations. All statistical analyses were performed using SPSS 21.0 (SPSS Korea Data Solutions, Seoul, Korea). Statistical significance was defined as a p-value lower than 0.05. Comparisons of numerical variables between groups were performed using the unpaired t-test. In comparisons between the pre- and post-closure states of patients, paired t-tests were used, and additionally, analysis of covariance adjusted for heart rate was performed. Simple linear regression analyses were used to determine any correlations between the deformation values and their procedural differences (pre-closure values minus post-closure values), and the parameters obtained from the catheterization results. Chi-square tests were performed to analyze gender distributions. To detect variables which present with gender differences, unpaired t-tests were performed between genders in the control subjects.
Results
Twenty seven excluded patient with incomplete echocardiographic images were not different from 114 subjects with ASD in demographic findings including age (p = 0.644), and in data of catheterization including Qp/Qs (p = 0.584) and RVEDP (p = 0.545). The demographic findings of the patients and controls are presented in Table 1. There is a significantly greater number of females in the patient group (p = 0.003). However, no another demographic or echocardiographic variables were significantly different between two genders (data not presented).
The results of the echocardiographic examinations of the patients, pre- and post-closure, and the controls are presented in Table 2 and Fig. 2. In ASD patients, mean iRVLD was reduced post-closure (p < 0.0001), and there was no significant difference between the mean iRVLD in post-closure ASD patients and controls (p = 0.160).
The mean values of єBL and SRBL were not different between pre-closure patients and controls (p = 0.245, p = 0.866); however, in patients, these values were decreased after closure (p = 0.001, p = 0.018). In ASD patients, the mean values for єAL and SRAL were also decreased after closure (all p < 0.001); however, these values pre-closure were higher than those in controls (p = 0.001, p < 0.001). Mean єBL in post-closure ASD patients was lower than that in controls (p = 0.001). Comparisons of unadjusted deformation values between groups showed similar tendencies of values, except several different results of statistical significances.
Using an analysis of covariance adjusted for heart rate which undergone due to the difference of heart rate between pre- and post-closure ASD patients, the mean values of SRB (p = 0.021), SRBL (p = 0.016), and SRAL (p = 0.045) remained significantly different between pre- and post-closure ASD patients.
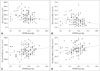
Qp/Qs was 2.71 ± 1.09, RVEDP was 8.6 ± 3.2 mm Hg, and mean pulmonary artery pressure was 18.9 ± 4.2 mm Hg in ASD patients. Qp/Qs was significantly associated with the procedural differences of єBL (p = 0.017) (Table 3) and SRBL (p = 0.019). RVEDP was significantly negatively associated with post-closure єBL (p = 0.020) and post-closure SRBL (p = 0.012), and it was positively associated with the SRBL procedural difference (p = 0.027) (Fig. 3). Mean pulmonary arterial pressure was negatively associated with the procedural difference of SRAL (p = 0.028).
Discussion
Myocardial deformation is not only dependent on myocardial contractility, but also dependent on ventricular dimension and preload/afterload.9)17)23) In this study, we adjusted measured values of RV deformation to indexed longitudinal RV length and we expected the correction of the effect of increased RV dimension. We assumed RV deformation values in post-closure state in which RV preload completely removed would reflect RV contractility and remodeling from chronic volume overload. Additionally, we assumed that procedural differences of RV deformation would reflect immediate preload dependence of RV in ASD patients. Resultantly, RV deformation values in pre-closure state would reflect both RV remodeling from chronic volume overload and immediate preload dependence of RV. Regression analysis showed that Qp/Qs was correlated with procedural differences of RV basal deformation and that RVEDP was correlated with post-closure basal deformation. These results suggest the dependence of the deformation of RV basal free wall and its remodeling on RV preload in spite of low correlation coefficient values.
In this study, we used a two segmental approach, by dividing the RV free wall into apical and basal segments. This two segmental approach has been applied in another studies,10)16)19) and seems to be reasonable in a longitudinal segmental analysis of RV deformation because anatomically the RV has three parts, the inlet, the trabecula, and the infundibulum of which two can be examined on an apical four-chamber view. In healthy individuals, the deformation of the two segments of the RV free wall is not different.24) However, the behaviors of the two segments were found to be different in this study in common with other reported study design which segmental approach used for analyzing RV deformation in patients with RV illnesses.10)16)17)19)
The basal segment deformation values in pre-closure ASD patients were higher than those in post-closure, and were not different from those of controls. The lower post-closure values may be the result of RV basal free wall remodeling, and the higher pre-closure values may be due to compensation caused by the increased preload. Decreased deformation of RV basal segments has been observed in extreme athletes.25) This might be the result of adaptation to chronic loading conditions, and seems to be equivalent to the results seen in post-closure patients in this study. Di Salvo et al.19) also reported decreased RV basal segment deformation in post-closure patients, and reverse remodeling of the basal segment might not be achieved until 6 months post-closure as all their subjects underwent ASD closure more than 6 months before their study.
Increased deformation of the RV apical segment in pre-closure ASD patients has been reported, and has been assumed to be the result of RV loading.16)17)18)20) Van De Bruaene et al.16) showed that RV apical segment deformation was significantly correlated with preload-linked echocardiographic variables. In this study, apical segment deformation values in pre-closure patients were found to be higher than those in post-closure, and were also higher than in controls. However apical deformation values in post-closure patients were not found to be different from those of controls, as has been described in other studies where percutaneous device insertion was used for ASD closure.19)20) In one study, decreased post-closure apical deformation was observed only in patients who had undergone surgical closure.19) Therefore we assumed that the remodeling of RV apical segment from chronic volume overload is not significant in ASD patients, and that the increased deformation values in apical segment may be from immediate preload dependence. Unfortunately, we could not found significant correlation between apical segment deformation values and the preload-linked variables that were determined by catheterization. However, a significant correlation was observed between procedural difference of SRAL and mean pulmonary arterial pressure. This relation suggests a possibility of the dependence of RV apical segment on the afterload at least partly in ASD patients. In patients with pulmonary hypertension, Dambrauskaite et al.10) demonstrated a prominent dependence of apical deformation on the afterload. The dependence of RV apical segment on afterload possibly deranged the identification of correlation between the deformation of RV apical segment and preload in this study.
In this study, we observed that the mean heart rate was different between pre- and post-closure ASD patients. However, this confounding factor may not invalidate the interpretation of the procedural differences of RV deformation results, as similar results were obtained in comparisons of pre- and post-closure SR values using analysis of covariance adjusted for heart rate although which cannot support a comparison of paired data.
This study had meaningful limitations. Thus far, several explanations for the basal-apical RV deformation differences in ASD patients has been suggested in one previous study; different wall thickness between the two segments, altered geometry of RV, and altered distribution of adrenergic receptors in RV.16) However, this study cannot add any further details to the above explanations. To investigate the differential behaviors of the two segments of the RV in ASD patients, we recommend a study using cardiac magnetic resonance imaging with which an accurate investigation of segmental volumes and wall motions is possible.
Different sedative conditions between in echocardiography and in catheterization also a limitation.
In conclusion, the longitudinal deformation of the RV basal segment is dependent and its remodeling is also dependent on volume loading in children with ASD.





 XML Download
XML Download