

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Brucellosis is a multi-systemic zoonotic infection which is common in the Middle East, Central Asia, the Mediterranean basin and Central America.
Although brucella endocarditis is an uncommon complication, it remains the main cause of brucellosis-related mortality.
Here we report the clinical and transesophageal echocardiographic findings of an interesting case with brucella endocarditis of an aortic root pseudoaneurysm following Bentall operation.
Case
A 40-year-old veterinarian with bicuspid aortic valve developed type A aortic root dissection following hypertensive crisis and underwent Bentall operation a year ago. His past medical history was positive for an episode of treated brucellosis.
Four months after the operation, he complained of fever, malaise, arthralgia of the left hip joint, anorexia and weight loss. The erythrocyte sedimentation rate was 103, Wright = 1/1280 and 2-mercaptoethanol (2ME) = 1/320. Combination antibiotic therapy with rifampin 900 mg/day per os (PO), doxycycline 200 mg/day PO and ciprofloxacin was started and continued for 6 months resulted in disappearance of his symptoms. Then after he was well untill about 14 days prior to his recent admission, when he again developed hip pain, fever, shortness of breath, profound fatigue and weakness. The erythrocyte sedimentation rate was elevated, his 2ME increased from 1/320 to 1/640. Because of recurrence of brucella symptoms, a transthoracic echocardiogram was done which showed a competent non-stenotic prosthetic aortic valve with no vegetation. The mitral and tricuspid valves were normal; however, there was question of vegetations attached to the inner surface of the Dacron wall. BACTEC blood cultures × 5 were obtained and he was empirically started on multiple antibiotics including doxycycline.
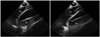
At this time the patient was transferred to our university hospital. His chest X-ray showed mild cardiomegaly and blunting of right costophrenic angle. Sinus tachycardia, left anterior hemiblock and non-specific ST-T wave changes in lateral leads were found in his initial electrocardiogram. An emergency transesophageal echocardiogram and color Doppler mapping revealed the detachment of valve-conduit from the annulus and the mitral-aortic intervalvular fibrosa and a large aortic pseudoaneurysm with multiple sessile and mobile vegetations attached to its Dacron walls (Fig. 1 and 2, Supplementary movie 1).
The prosthetic aortic valve appeared to have normal motion and to be free of any vegetation. No aortic regurgitation was noted either (Fig. 2). Color-flow imaging showed the entrance of most of the cardiac stroke volume into a large pseudoaneurysm covering almost the entire circumference and length of the Dacron graft as far as it could be seen (Fig. 1 and 2, Supplementary movie 1). The next day, he underwent an un-eventful redo operation. A huge pseudoaneurysm was detected at surgery and the whole valve-conduit was replaced with a 25 mm homograft. His condition improved and he was discharged on day 7, in a stable condition. Before discharge, the initial blood and vegetation cultures were reported to be positive for rifampin-resistant Brucella melitensis. He was treated with doxycycline 200 mg/day PO, plus ciprofloxacin and gentamicin 5 mg/kg/day intramuscularly for 14 days. Subsequently he received the same dose of doxycycline for several additional months.
Discussion
Our patient had a unique presentation namely Brucella endocarditis of a pseudoaneurysm of an aortic composite graft. Endocarditis following Bentall operation is quite rare and life threatening if untreated.1)
Brucellosis is a systemic disease mainly affecting the musculoskeletal system. Cardiovascular complications, including endocarditis, are rare but usually fatal. The aortic valve is most often involved. This includes both the native and prosthetic valves.
Brucella infection was considered as the possible underlying cause for the dehiscence of the conduit from the aortic annulus and formation of pseudoaneurysm in our patient.2)
Infection of a prosthetic cardiac device is a rare complication of brucellosis; however, it should be highly considered in any case with recurrent symptoms such as our patient.
Overall, early diagnosis and prompt medical and surgical interventions are essential for patients' survival3) since endocarditis continues to be the principal cause of mortality in the course of the disease.
Transesophageal echocardiography and color Doppler mapping have become the most popular non-invasive, cost effective and easy-to-do procedure of choice for detection of the complications associated with Bentall procedure and composite grafts. These include pseudoaneurysms, which may occur in 7% to 25% of cases, supravalvular aortic stenosis, which occurs less often4)5) and endocarditis, which is the least frequent complication and was observed in our patient.
In conclusion, this rare case report is additive to the previously reported albeit, infrequent complications of Brucella-induced cardiac prosthetic endocarditis.6)
It emphasizes the need for a high clinical suspicion in susceptible cases, particularly those with recurrent brucellosis and shows the utmost importance of transesophageal echocardiography for the diagnosis and guiding of therapy in such patients.

 XML Download
XML Download