

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiovascular disease accounts for 35-50% of all cause mortality in kidney transplant recipients. Among transplanted kidney patients, cardiovascular disease mortality rates are at least two-fold higher than an age stratified sample of the general population but significantly lower than an age stratified dialysis population.1) Detection and follow-up of cardiac abnormalities in patients with end stage renal disease therefore plays an important role in clinical practice.
It has become apparent that torsion or twisting motion of the left ventricle (LV), which results from rotation of the apex and base of the heart in different directions, is integral to normal cardiac function. LV rotation plays an important role in maintaining efficient myocardial contraction during systole and aids in generating early suction power during the isovolumic relaxation period.2)3) Assessment of rotation may provide important insights into different types of myocardial dysfunction and the effect of different treatment strategies.4-9) Recent technological advances in echocardiography such as velocity vector imaging allows for the quantification of myocardial mechanics including rotation, twist and torsion.
Prior studies have reported anatomic and functional abnormalities in kidney transplant recipients,10)11) but the effects of kidney transplant on LV rotation, twist and torsion has never been investigated. Therefore, we employed velocity vector imaging to assess LV rotation, twist and torsion pre and post kidney transplant in end stage renal disease patients without myocardial infarction.
Methods
Subjects
Sixty end stage renal disease Caucasian patients (12 female) aged 36-67 years who had undergone a renal transplantation were prospectively enrolled. Repeat echocardiography was performed 6 months after transplant surgery. Exclusion criteria were: 1) lack of immediate graft function; 2) early graft loss within the first three months of renal transplantation; 3) known cardiac infarction, valvular, ischemic or nonischemic cardiomyopathy, congestive heart failure and arrhythmias; and 4) previously diagnosed sleep-apnea syndrome. We excluded subjects with any known co-morbidity that may influence myocardial function. Forty-eight patients met inclusion criteria. Comorbidities among the group included: hypertension (n = 36), diabetes mellitus (n = 20), and treated coronary artery disease (n = 24). Demographic, anthropometric and biochemical data included height, weight, blood pressure, blood urea nitrogen (BUN), creatinine, hemoglobin, electrocardiogram and echocardiography prior to and six months post kidney transplantation. The study protocol was approved by the Mayo Clinic Institutional Review Board and the subjects provided the informed consent.
Echocardiography
All subjects underwent a standard complete 2-dimensional, Doppler echocardiography and tissue Doppler imaging with an Acuson Sequoia C512 ultrasound system (Siemens Medical Solutions, Inc., Mountain View, CA, USA) with a 3.5 MHz transducer. Scans included: 1) apical 2-chamber and 4-chamber views for measurements of LV ejection fraction (LVEF); 2) short-axis apical and basal views for analysis of rotation by velocity vector imaging and calculation of torsion magnitude; 3) flow Doppler spectra with early (E-wave) and late (A-wave) component of LV filling measured by positioning the sample volume at the level of the tips of mitral leaflets in the apical 4-chamber view; and 4) tissue Doppler of early peak diastolic mitral annulus velocity (e') measured at the basal medial annulus. Images of three cardiac cycles were acquired with a frame rate > 70 Hz. The LVEF was calculated by the modified Simpson's method.12) Early diastolic myocardial velocity was measured at the medial mitral annulus. LV mass was estimated from LV linear dimensions as: LV mass = 0.8 × {1.04 [(LVIDd + PWTd + SWTd) - (LVIDd)]} + 0.6 g. Where LVIDd is LV internal dimension at end diastole, PWTd and SWTd are posterior wall thickness at end diastole and septal wall thickness at end diastole, respectively. LV mass was indexed by body surface area. Relative wall thickness at end of diastole (RWtd) was calculated by the formula (2 × PWTd) / LVIDd. All measurements were performed according to the guidelines of the American Society of Echocardiography.12)13)
Velocity vector imaging
Syngo velocity vector imaging technology software (Siemens Medical Solutions, Inc., Mountain View, CA, USA) was used offline to track endocardial motion. The apical and basal short-axis images were converted into uncompressed Digital Imaging and Communications in Medicine format for subsequent velocity vector imaging analysis. To minimize inter-observer variability, a single experienced observer, blinded to the subject's data, performed all tracing. An optimal frame was selected where the basal or apical endocardial definition was well seen, to allow clear endocardial border tracing. The best endocardial definition is usually in the mid to late systolic frames. Where good endocardial definition is noted, points are placed on the endocardium close to the myocardium. An average of 7 points per trace was defined. In the basal short axis views, a frame is selected that clearly separates the mitral valve from the endocardial border, to avoid tracking the valve. The trace is started at the 12 o'clock position. Tracking results are selected only when the tissue is followed accurately. LV rotations at the basal or apical short-axis views were determined as average angular displacement of 6 myocardial segments. The positive peak of apical LV rotation and negative peak of basal LV rotation were automatically measured. Data points depicting the basal and apical LV rotation and rotational velocities were exported to Excel (Microsoft Corporation, Redmond, WA, USA) to calculate LV twist and torsion. LV twist is defined as the maximal instantaneous difference between the apical and basal rotations. LV torsion is defined for the purpose of this study as LV twist magnitude normalized to LV length.4)14)
All measurements are the averages derived from three consecutive cardiac cycles. The velocity vector imaging measurements were repeated in 10 subjects by the same observer and a second observer to determine the intra-observer and inter-observer correlations. Both of the observers were blinded to subjects
data.
Statistical analysis
The SPSS version 13.0 software (SPSS Inc., Chicago, IL, USA) was used for the statistical analyses. Categorical data were expressed as frequencies. Continuous data were expressed as mean ± standard deviation. Comparison of continuous variables was performed by paired t-test. Comparison of categorical variables was performed by the chi-square test. Correlation between velocity vector imaging parameters and other data was tested by Spearman correlation coefficients. Linear stepwise regression was performed to assess the adjusted association. Statistical significance was defined as p <0.05. Interclass correlation coefficient was used for evaluation of reproducibility.
Results
Patient characteristics
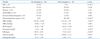
The basic characteristics of the groups are shown in Table 1. Systolic blood pressure, heart rate, BUN and creatinine post kidney transplantation were significantly lower than pre kidney transplantation (p < 0.05). Glucose was higher than pre kidney transplantation (p < 0.05). The distribution of cardioactive drugs was not statistically significant different pre- and post kidney transplantation. The noted change were that only two patients were on erythropoiesis stimulating agent after transplantation, compared with 52% of those before transplantation and all the patients were on immueosuppressive agents after transplantation. There was no significant difference in hemoglobin pre and post kidney transplantation (p > 0.05).
Conventional echocardiography
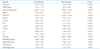
LVEF, ratio of mitral early and late diastolic filling velocity, and LV rotation, twist and torsion were increased significantly post kidney transplantation compared to pre kidney transplantation (p < 0.05) (Table 2). Interventricular septum thickness, left ventricular mass index, systolic blood pressure, serum blood urea nitrogen and creatinine were decreased significantly post kidney transplantation compared to pre kidney transplantation (p < 0.05). There was no significant difference pre and post kidney transplantation in RWtd (p > 0.05) (Table 2). Based on data in Table 2, LV displayed concentric hypertrophy pre and post kidney transplantation in end stage renal disease.
Velocity vector imaging
Post kidney transplantation peak rotation of apical LV (ROT-API), peak rotation of basal LV (ROT-BAS), peak twist (TW) and peak torsion of LV (TOR) were significantly higher than pre kidney transplantation (p < 0.05) (Fig. 1, Table 2). There was no significant difference between absolute value of ROT-BAS and ROT-API (p > 0.05). Peak TOR was positive correlation with E, A, E/A, e, LVEF, ROT-API, ROT-BAS, TW (0.65, 0.25, 0.6, 0.4, 0.49, 0.83, 0.77, 0.83, respectively, p < 0.05). Peak TOR was negative correlation with mitral E wave deceleration time (DT), interventricular septum (IVS), LV mass index (LVMI) (-0.31, -0.34, -0.77, respectively, p < 0.05). There was no independent predictor for improvement before kidney transplantation.
Discussion
This study demonstrated that kidney transplantation resulted in improvement of left ventricular structure, function and torsion after 6 months transplantation. To our knowledge, this was the first study to focus on left ventricular torsion pre and post kidney transplantation.
This study showed that conventional echocardiographic indices of LV function, including LVEF and E/A were improved within 6 months after kidney transplantation. In our study, E/A ratio was significantly increased after kidney transplantation, but E/e' was not changed significantly. And there was e' < 0.08 m/s, which indicated left ventricular diastolic dysfunction. Our results were in accordance with prior studies, and indicated the left ventricular diastolic function was improved, but still abnormal. LV structure also showed improvement of interventricular septum thickness and left ventricular mass. In general, correction of the uremic state by renal transplantation leads to improvement of LV structure and function. Prior studies, not using VVI technology, demonstrated that there were structural and functional improvements in cardiac indices post kidney transplantation.15)16) Wali et al.15) reported that kidney transplantation in end stage renal disease patients with advanced systolic heart failure resulted in an increase in LVEF.
Compared to pre kidney transplantation, ROT-BAS, ROT-API, TW and TOR were significantly higher post kidney transplantation, indicating an improvement in overall myocardial mechanical function, but there was no significant difference between absolute value of ROT-BAS and ROT-API. It has been established that in healthy subjects rotation of the LV base is opposite to that of the apex but is significantly lower in its magnitude. In the normal heart, the counterdirectional rotation of the LV apex with respect to the base results in a wringing movement during ejection. The rotation angle increased with distance from base to apex, and subendocardial rotation was found to be higher than subepicardial rotation.17)18) The pattern of net LV twist in which the apex and the base rotate in different directions has been explained on the basis of varying spiral myofiber architecture of the apical and basal region and apex-to-base and transmural gradients in myosin phosphorylation.19-21) For optimal cardiac mechanical function it is important to maintain rotation of the LV apex in a direction opposite to and higher than the base. Our study shows an improvement of rotation, twist and torsion post kidney transplantation, rotation of the LV base was opposite to that of the apex but was higher in its magnitude, and the left ventricular rotation pattern was still different from normal subjects.
Physiological variables such as preload, afterload, contractility, exercise and age may influence the extent of LV rotation. The most important factors predisposing to abnormal cardiac performance and morphology in end stage renal diseases are systemic hypertension, anemia, volume overload, and in patients on hemodialysis, the arteriovenous fistula. Prolonged exposure to uremic toxins can result in myocyte fibrosis and cell death. Metabolic factors such as acidosis, hypoxia, hypocalcemia, and possibly high levels of parathyroid hormone, may impair LV function.22)23) Kidney transplantation is associated with a reversal of the biochemical toxins and conditions associated with uremia, which resulted in the improvement of LV structure, function and torsion.
In this study, peak TOR was positive correlation with E, A, E/A, e, LVEF, ROT-API, ROT-BAS, TW (0.65, 0.25, 0.6, 0.4, 0.49, 0.83, 0.77, 0.83, respectively, p < 0.05) and peak TOR was negative correlation with DT, IVS, LVMI (-0.31, -0.34, -0.77, respectively, p < 0.05). Studies of Kim et al.24) and Takeuchi et al.25) demonstrated similar results to confirm that left ventricular rotation varied with changes in preload, afterload, and contractility.
In our study, post kidney transplantation fasting glucose was higher than pre transplantation. Evidence suggested that immunosuppressive drugs accounted this, the association between immunosuppressive drugs and glucose increase had been established clearly and was related to cumulative dosages and therapy duration.26)
In this study, we performed myocardial rotation analysis by velocity vector imaging. Velocity vector imaging is not a simple speckle-tracking technique, as it uses a more sophisticated approach that involves endocardial border tracking performed with Fourier techniques that ensure higher accuracy using the periodicity of the heart's motion, which allows myocardial rotation to be accurately quantified for global and regional myocardial functional assessment.4)27)
However, this was a small number and single center study, and the effects of kidney transplantation on LV structure and function need long-term follow-up.
In conclusion, kidney transplantation in end stage renal disease without myocardial infarction results in improvement of LV structure, function, myocardial rotation, twist and torsion as detected by echocardiography and velocity vector imaging. Assessment of LV rotation, twist and torsion provided important insights into different types of myocardial dysfunction and the effect of different treatment strategies. Velocity vector imaging provided valuable information for detection and follow-up of cardiac abnormalities in patients with end stage renal disease.

 XML Download
XML Download